Chapter 181 Gastrointestinal Protectants
• Histamine-2 receptor antagonists (H2RAs) are competitive inhibitors of gastric acid secretion, meaning that they lower gastric acid secretion but do not abolish it. However, they also diminish pepsin secretion.
• Cimetidine inhibits hepatic P-450 cytochrome enzyme activity so much that it can be used therapeutically (e.g., to minimize acetaminophen toxicity) or can delay metabolism of drugs.
• Proton pump inhibitors (PPIs) are noncompetitive inhibitors of gastric acid secretion, meaning that they can inhibit gastric acid secretion to a greater extent than H2RAs. However, it can take 2 to 5 days for them to achieve maximal effectiveness when given orally.
• Sucralfate is an unabsorbed drug that binds to ulcerated or eroded mucosa. It can adsorb other drugs, delaying or inhibiting their absorption.
• Misoprostol is a prostaglandin analog that was designed to prevent ulceration and erosion due to nonsteroidal antiinflammatory drugs (NSAIDs). However, it is not as effective or reliable in preventing NSAID-induced ulceration in dogs as it is in humans.
INTRODUCTION
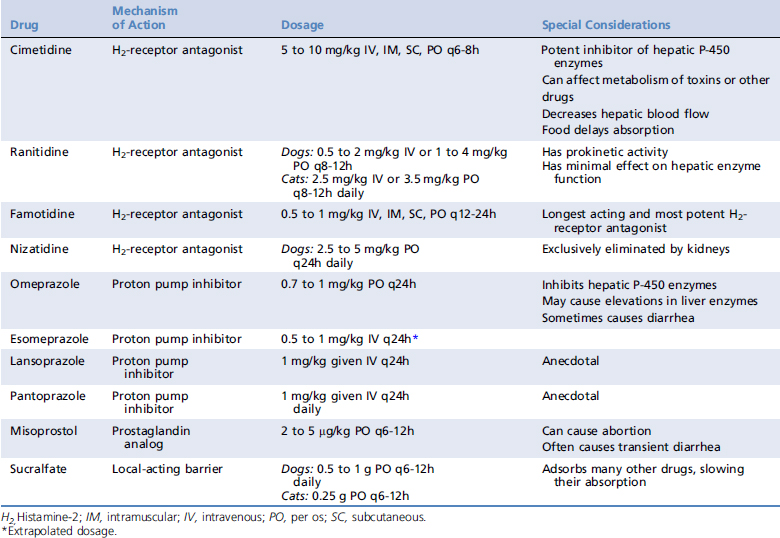
Gastrointestinal (GI) protectants are primarily indicated to heal existing gastric ulcers and erosions. Removing the cause of the ulceration or erosion markedly enhances efficacy, as does maintaining GI perfusion. Protectants are often poorly effective at preventing ulceration when the cause (e.g., use of NSAIDs, continued poor perfusion or anoxia to the gastric mucosa) persists. However, when there is a known cause of ulceration or erosion that cannot be readily alleviated, these drugs are often given in the hope that they will at least retard, if not prevent, ulceration. See Table 181-1 for a list of commonly used GI protectants and dosages.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


