G
Gastric Intubation, Gavage, Lavage
INDICATIONS
• Gastric intubation:
○ Preoperative stabilization of gastric dilatation/volvulus (GDV); allows evacuation of gas and fluid, resulting in an improved hemodynamic state
• Lavage:
○ Preoperative stabilization of GDV. Removal of stomach contents may help decrease the speed of gas reaccumulation while the animal is being prepared for surgery, thus slowing or preventing cardiovascular deterioration.
CONTRAINDICATIONS
• Esophageal disease that could lead to tube-induced trauma or perforation. Conditions of concern include esophageal stricture, neoplasia, ulceration, megaesophagus, and recent esophageal surgery.
• Gastric disease that could lead to tube-induced trauma or perforation. Conditions of concern include neoplasia, ulceration, and recent gastric surgery.
• Any swallowing disorder (megaesophagus, esophageal motility disorder, etc.), pharyngeal disorder, or laryngeal disorder (paralysis, previous tie-back surgery, etc.) that could predispose a nonendotracheally intubated animal to aspiration.
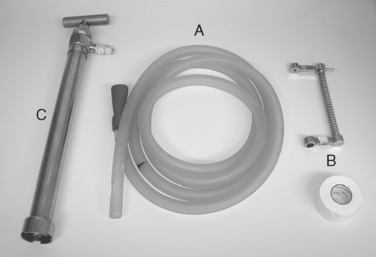
EQUIPMENT, ANESTHESIA
• Flexible plastic tubing of various length and diameter. The distal end must be smooth and atraumatic; smoothing may be achieved by brief heating of the end of the tube over a flame, cooling, and trimming edges with a scalpel blade. One to three side holes may facilitate evacuation of stomach contents by minimizing obstruction of a single distal hole with gastric mucosa or ingesta.
If gastric lavage, all of the above, plus:
PREPARATION: IMPORTANT CHECKPOINTS
• Ensure that adequate manual or chemical restraint for the procedure is planned. Personal preference and animal stability may dictate the degree of sedation or anesthesia chosen. Note: Some clinicians prefer to ensure a patent and protected airway to minimize the potential for aspiration pneumonia through the use of general anesthesia and a cuffed endotracheal (ET) tube when gastric lavage is performed.
POSSIBLE COMPLICATIONS AND COMMON ERRORS TO AVOID
• Inadvertent passage of the orogastric tube into the trachea can result in mild to severe complications:
○ Tracheal or bronchial placement of the gastric tube can result in airway obstruction until the tube is repositioned.
○ Tracheal or bronchial administration of gavage or lavage fluids can result in severe aspiration pneumonia and death.
• Oral, pharyngeal, laryngeal, esophageal, or gastric trauma can result if excessive force is used for passing the gastric tube. Full-thickness tearing is possible, especially with a preexisting underlying disease.
• Inability to pass the tube into the stomach may be due to the choice of a tube with a diameter that is too large, esophageal obstruction (foreign body, stricture, neoplasia), torsion of the stomach, or excessive lower esophageal sphincter (LES) tone. Discontinuation of metoclopramide prior to elective gastric intubation is recommended to minimize LES tone.
• Inadequate sedation of an uncooperative animal will lead to longer procedure times and increased risk of injury to the animal and veterinary staff.
• Inability to effectively remove gastric contents through lavage may be related to excessive size or adhesive nature of gastric contents, gastric compartmentalization, or other factors.
• Regurgitation during lavage, gastric overfilling, or esophageal administration of large volumes of lavage fluid can result in aspiration if a cuffed ET tube is not in place.
• Excessive tube advancement can cause occlusion of the distal end of the tube against stomach mucosa. Palpation of the tube pressing against the stomach wall may indicate a need for partial retraction.
PROCEDURE
• Position animal in sternal recumbency. If animal is uncomfortable, alternate positions may be better tolerated (sitting, standing, lateral, etc.).
• Choose appropriate tube diameter for esophageal size and procedure planned. Example: A tube with an outer diameter of 1.5 inches (3.5 cm) is appropriate for most medium-sized dogs (45 lb [20 kg]). A larger tube size may be necessary for effective lavage versus gas decompression.
• Measure the length of tube necessary to pass from the nose to the xiphoid. Mark this distance on the tube with a piece of tape or nontoxic marker.
• Place a mouth gag (speculum) to prevent the animal from chewing on the tube.
○ A roll of 2-inch (5 cm)-wide clinic-type white cloth tape works well in many animals. The tube will pass through the hole in the tape roll. Place tape roll on top of the tongue and behind all 4 canine teeth.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


