5 Flea allergic dermatitis
CASE HISTORY
• Long-standing history of non-seasonal pruritus involving face, feet and ventrum, and more recently the dorsal trunk had also become involved.
• The pruritus has been managed with intermittent methylprednisolone acetate injections, but these had become ineffective with severe deterioration in the dog’s clinical condition.
• The dog was mainly fed on a commercial pet food and more recently an 8-week diet trial with a prescription hydrolysed hypoallergenic diet had failed to resolve the pruritus or the clinical lesions.
• The three in-contact cats were unaffected and were intermittently treated for fleas with a pet shop product.
CLINICAL EXAMINATION
The clinical findings in this case were:
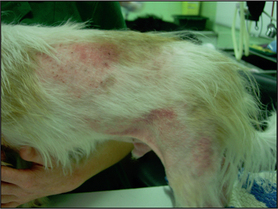
• Severe generalized erythema with papules, follicular papules and crusted patches on the trunk (Figs 5.1 and 5.2).
• The periocular skin was hyperpigmented, lichenified and erythematous, with evidence of excoriations (Fig. 5.4).
• Erythema, self-induced alopecia, crusting and hyperpigmentation involving all four feet (Fig. 5.5).
• The peripheral lymph nodes were not enlarged and the other physical parameters were within normal limits.




CASE WORK-UP
A number of the differential diagnoses were ruled out with simple in-house tests:
• Skin scrapes were performed to rule out demodicosis and to look for sarcoptic mange. Negative skin scrapes do not definitively rule out sarcoptic mange and therefore a Sarcoptes IgG ELISA test was performed, which was also negative.
• There was no fungal growth after 3 weeks of culturing of a sample obtained by the MacKenzie toothbrush technique.
• Tape-strip samples, obtained from crusted lesions, revealed clumps of coccoid bacteria, neutrophils and keratinocytes.
• Staphylococcus intermedius was isolated from a swab submitted for bacterial culture, which was sensitive to amoxicillin/clavulanate, cefalexin, enrofloxacin, marbofloxacin, clindamycin and trimethoprim/sulphonamide. It was resistant to amoxicillin, penicillin and tetracycline.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


