11 Adverse food reaction
CASE HISTORY
CLINICAL EXAMINATION
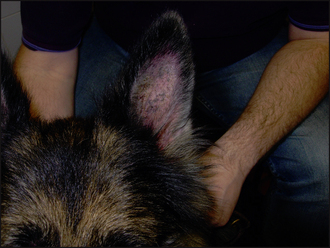
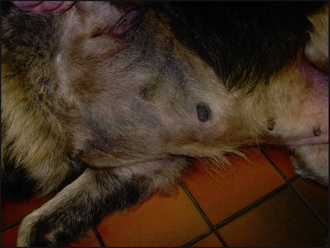
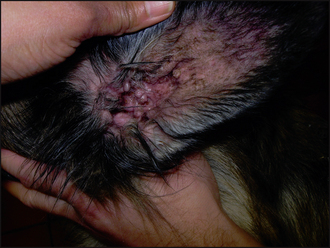
The clinical signs of adverse food reactions are variable and range from non-lesional pruritus to severe self-induced excoriations and ulceration. The lesion distribution may be localized, such as an acral lick dermatitis in large breeds of dogs, or generalized. The most common primary signs are erythema and papular reactions. Secondary lesions include excoriations, crusts, lichenification, hyperpigmentation and scaling. Secondary recurrent bacterial pyoderma and Malassezia dermatitis is common. Recurrent otitis externa and/or media are reported in up to 80% of dogs with an adverse food reaction.

The differentials considered for the underlying causes of pruritus (i.e. primary diseases) were:
The differentials considered for the secondary condition were:
CASE WORK-UP
In this case, the following tests were performed at the first visit:
Ectoparasitic disease was ruled out on the basis of the negative tests and ectoparasitic therapy. The clinical signs and the initial laboratory findings confirmed the involvement of a secondary superficial staphylococcal pyoderma and otitis externa. Empirical treatment for pyoderma and otitis was started immediately (clindamycin 10 mg/kg b.i.d.; daily acetic acid/boric acid ear cleaning and twice daily applications of a fucidic acid-containing product). The case was reassessed after 4 weeks, at which time the pyoderma and otitis had resolved (Figs 11.4 and 11.5), but pruritus persisted. In addition, the concave aspects of the pinnae and ventral inguinal skin were still mildly erythematous, supporting a probable allergic component. The next stage was to start a diet trial to investigate the involvement of an adverse food reaction.

Diet trials
Choice of diet: There are two choices of food, either novel protein and carbohydrate (i.e. ingredients to which the animal has not previously been exposed) or a hydrolysed protein. The selection of ingredients for a novel protein diet is based on the previous dietary history. Unfortunately, more often than not the exact ingredients within a commercial diet are unknown. In the UK, chicken, beef and wheat are common ingredients in dog foods, while fish, chicken and wheat are common ingredients in cat foods. Treats and table scraps given to the pet should also be taken into account. Hydrolysed diets usually contain chicken or soy protein that has been enzymatically degraded to break large protein molecules into smaller peptide molecules, rendering them, in theory, non-immunogenic. Although undoubtedly convenient, there is still a lack of data in veterinary dermatology as to whether dogs allergic to the parent protein will not react to the hydrolysed molecule. Novel protein and carbohydrate diets may be either home-cooked or proprietary preparations. All other foodstuffs including treats, chews, flavoured toys and toothpastes should be avoided. The choice of which diet to feed is based on an assessment of the previous dietary history and a discussion of the implications of the various options with the owner. In general, it is good practice to feed a type of diet which maximizes owner compliance. Although home-cooked diets are considered to be the ‘gold standard’, ultimately clients often find home cooking too much of a chore. Owner compliance is the major limitation in dietary trials.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


