Chapter 6 Eyelids
ANATOMY, FUNCTION, AND PATHOLOGIC RESPONSES
Anatomy and Function
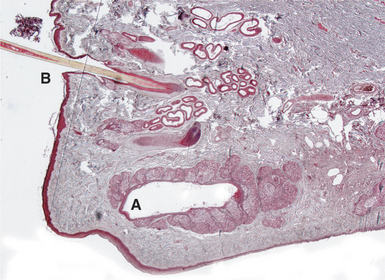
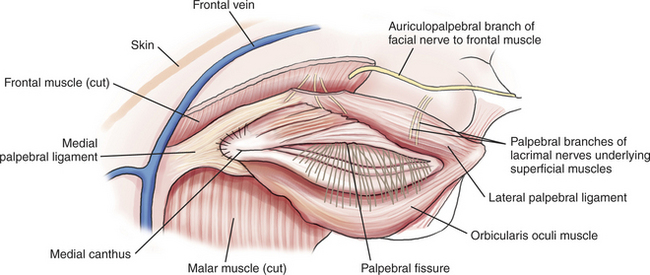
The eyelids consist of a fibrous tarsal plate and muscle, bounded by skin on the outer surface and conjunctiva on the inner surface (Figure 6-1). In addition, there are a number of adnexal specializations, such as cilia (eyelashes) and glands. These components vary by species; however, some general comments are possible. The skin on the outer surface of the eyelid is thinner, more mobile, and more pliable than skin elsewhere on the body. Cilia are present on the outer surface of the upper eyelid margin in dogs, horses, cattle, pigs, and sheep. A few cilia also are present on the lower eyelids of horses, cattle, and sheep. Cats have no cilia but do have a line of modified hairs that are essentially identical. Modified sweat glands—the glands of Moll—open onto the eyelid margin near the base of the cilia. The glands of Zeis are rudimentary sebaceous glands that open into the follicles that produce the cilia. The tarsal or meibomian glands (Figures 6-1 and 6-2) are modified sebaceous glands that are embedded in the tarsal plate, a layer of fibrous tissue that gives some structural rigidity to the eyelid. The meibomian glands open right at the eyelid margin posterior to the cilia. Their orifices are visible grossly, and a grayish white secretion rich in phospholipids can be expressed from them. This secretion has two functions: It coats the eyelid margins to minimize overflow of tears and it forms the superficial lipid layer of the precorneal tear film. This lipid layer has high surface tension and thereby adds stability to and reduces evaporation of the aqueous layer of the tear film.
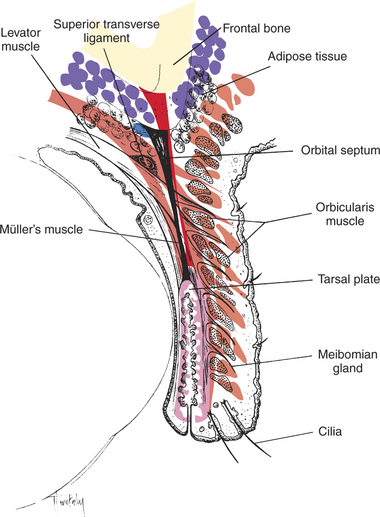
Figure 6-1 Anatomy of the normal eyelid.
(From Remington LA [2005]: Clinical Anatomy of the Visual System, 2nd ed. Butterworth-Heinemann, St. Louis.)
Tear film components drain from the ocular surface through the lacrimal puncta, which lie on the inner surfaces of the upper and lower eyelids 3 to 4 mm lateral to the medial canthus, approximately opposite the last of the meibomian gland openings. The lacrimal canaliculi drain into the lacrimal sac, which lies in a fossa of the lacrimal bone. Blinking creates a negative pressure within the sac, thereby drawing tears into it. During the relaxation phase of blinking, pressure is placed on the sac, thereby forcing tears down the nasolacrimal duct. This forms the so-called lacrimal pump. Blinking occurs with contraction of the orbicularis oculi muscle, which encircles and closes the palpebral fissure (Figures 6-3 and 6-4). It is innervated by the palpebral nerve, a branch of the facial nerve (cranial nerve [CN] VII) (Figure 6-5). Localization of this nerve is important for injection of local anesthetic and induction of akinesia of the upper eyelid in large animals.
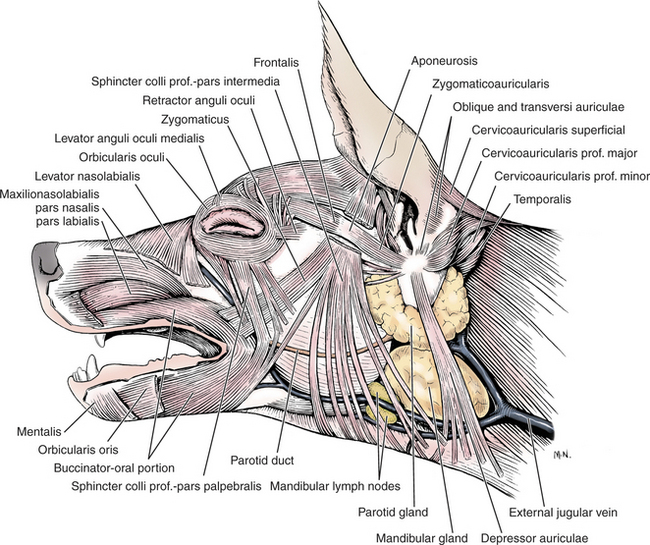
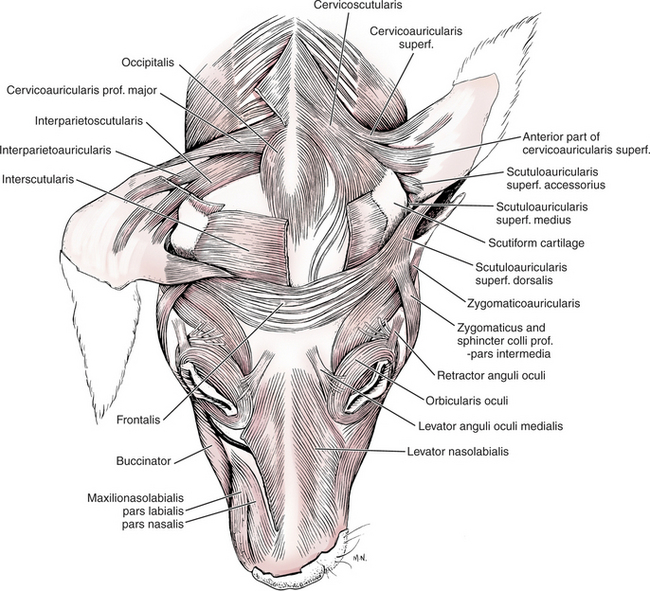
Figure 6-4 Dorsal view of the deep muscles of the canine head.
(Modified from Evans HE [1993]: Miller’s Anatomy of the Dog, 3rd ed. Saunders, Philadelphia.)
The general pattern and innervation of muscles surrounding the eyelids is similar in all species, although the names and relative development differ somewhat among species. The orbicularis oculi muscle is the major muscle responsible for eyelid closure. It is anchored medially to the wall of the orbit by the medial palpebral ligament (see Figure 6-5) and laterally by the retractor anguli oculi lateralis (see Figures 6-3 and 6-4). In cattle and sheep this latter structure is fibrous in nature and is known as the lateral palpebral ligament (see Figure 6-5). In horses it is visible as a fibrous raphe within the orbicularis muscle. The medial and lateral attachments of the orbicularis oculi preserve the elliptical shape of the palpebral fissure and prevent it from becoming circular during contraction of the orbicularis. Excessive muscle tone in the orbicularis oculi muscle, called blepharospasm, may result in spastic entropion.
Opening of the eyelids requires not only relaxation of the orbicularis oculi muscle but also elevation of the upper eyelid and depression of the lower eyelid. The upper eyelid is more mobile than the lower eyelid in mammals, although the opposite is true in birds and reptiles. The major elevators of the upper eyelid are the levator palpebrae superioris, which originates near the optic foramen, inserts into the tarsal plate, and is innervated by the oculomotor nerve (CN III), and Müller’s muscle, which lies posterior to the levator and is sympathetically innervated (see Figure 6-1). The levator and superior rectus muscles have common innervation (CN III), so that elevation of the globe by the superior rectus muscle is coordinated with elevation of the upper eyelid. If it were not, the animal would see the inner surface of the upper eyelid on elevation of the globe. The levator anguli oculi medialis and frontalis muscles are minor elevators of the upper eyelid and are both innervated by the palpebral nerve (see Figures 6-3 and 6-4).
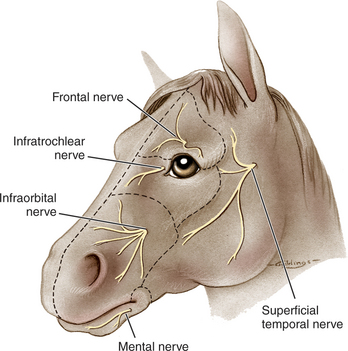
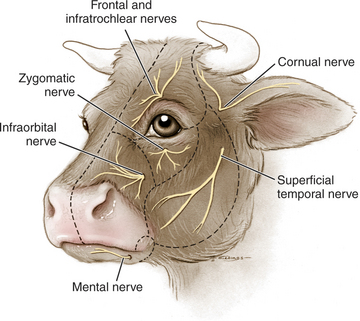
The lower eyelid is depressed by the malaris muscle, which is innervated by the dorsal buccal branch of the facial nerve. Note that different branches of the facial nerve supply the orbicularis, which narrows the palpebral fissure, and the malaris, which widens it. Actions of the muscles of the eyelids are summarized in Figure 6-6. Sensory innervation for the dog, horse, and ox is shown in Figures 6-7 to 6-9. Interference with sensory or motor innervation of the eyelids may result in severe desiccation of the cornea and conjunctiva.
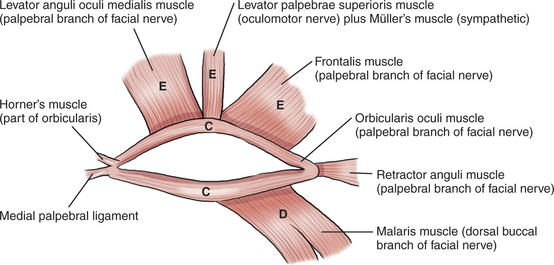
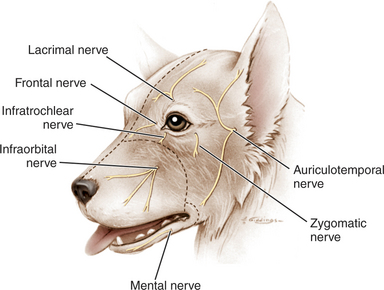
Figure 6-7 Sensory innervation of the canine periocular area.
(Modified from Westhues M, Fritsch R [1964]: Animal Anaesthesia, Vol 1: Local Anaesthesia. Oliver & Boyd, London.)
The eyelids protect the eye in the following ways:
DELAYED OR PREMATURE OPENING OF THE EYELIDS IN NEONATES
In the newborn foal or calf the eyelids are open at birth; whereas in the kitten and puppy they open at about 10 to 14 days of age. Premature opening occurs infrequently in dogs and cats but when it does, it results in corneal desiccation, keratitis, corneal ulceration, and conjunctivitis because tear production takes several weeks to reach adequate levels. If these consequences are left untreated, corneal perforation and endophthalmitis may occur. Treatment consists of frequent application of a topical lubricating ophthalmic ointment. Rarely, a temporary tarsorrhaphy may be necessary to further limit evaporation of tears and aid in corneal healing (see Chapter 10). A small gap should be left at the medial canthus to permit administration of bactericidal antibiotic or bland lubricating ointment. Sutures are removed after 7 to 10 days, but topical treatment may be necessary for a few days longer.
More commonly, delayed opening of the eyelids (ankyloblepharon) occurs in dogs or cats. This is often associated with accumulation of mucus and sometimes with infection (ophthalmia neonatorum). Typical infectious agents vary somewhat by species: Chlamydophila felis or feline herpesvirus is common in cats, and Staphylococcus spp. may infect dogs or cats. Ankyloblepharon can be treated conservatively with warm compresses for a short period in the expectation that the eyelids will open. However, if they do not open within a day or so, the eyelids should be gently pried open with firm digital pressure or by inserting the nose of a closed pair of small mosquito hemostats at the medial canthus, where there is often a small gap between the eyelids. The hemostats can then be gently opened in this position but should not be reclosed while inserted between the eyelids, so as to avoid damage to surface ocular structures. A sharp instrument should never be used for this purpose, and the fused eyelid margins should never be incised to separate them, because either action would cause irreversible damage to the eyelid margins themselves and/or the meibomian glands with subsequent lifelong keratitis. After the eyelids are pried apart, the ocular surface should be liberally irrigated with saline or dilute (1:50) povidone-iodine solution (not povidone-iodine scrub) and the cornea checked with fluorescein stain for evidence of ulceration. A topical antibiotic ointment with a spectrum appropriate for the suspected organisms should be applied a few times daily for approximately 1 week.
EYELID AGENESIS (COLOBOMA)
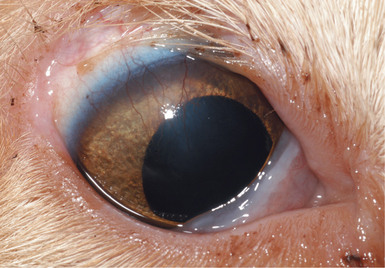
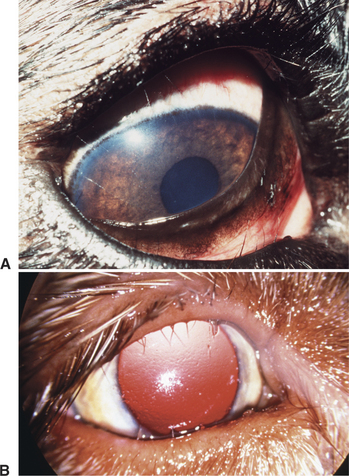
Eyelid coloboma refers to congenital absence of a portion of an eyelid. It can occur in all species but it is most common in cats, in which it usually affects the lateral portion of the upper eyelid (Figure 6-10). In piebald and Karakul sheep it has been described as affecting the middle of the upper eyelid. Coloboma is believed to be a hereditary condition. Dermoids may be seen in association with coloboma (see Chapter 10). Eyelid colobomas are associated with excessive evaporation and inadequate dispersion of the precorneal tear film, and sometimes with trichiasis. Together, these lead to secondary keratoconjunctivitis, pain, and sometimes corneal ulceration. If the lower eyelid is affected, epiphora may occur owing to escape of tears through the defect. With time, corneal scarring, pigmentation, and vascularization are common.
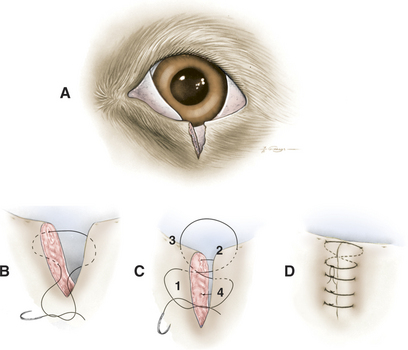
Eyelid colobomas are repaired with a variety of blepharoplastic procedures; the choice depends on the size and position of the defect. Larger defects require more extensive reconstructive procedures and are best referred to a veterinary ophthalmologist. However, simple defects affecting less than one third of the eyelid margin can be restored by removal of the edges of the defect so as to create a wedge defect (Figure 6-11). This is then closed in two layers with special care to accurately appose the sides of eyelid margin without leaving sutures that may abrade the cornea (Figure 6-12). Sutures are removed 10 days later. Postoperatively, an Elizabethan collar is used. The two-layer eyelid closure also should be used for reapposition of any incisions or lacerations involving the eyelid margin, including traumatic injuries, medial canthoplasty, tumor resection, and treatment of some cases of entropion or ectropion.
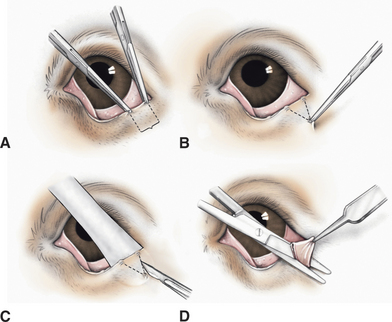
Figure 6-11 Eyelid wedge resection. This general technique may be used for correction of some cases of entropion or ectropion and smaller eyelid colobomas, freshening and closure of eyelid lacerations, and removal of eyelid tumors. A, The extent of eyelid margin to be resected may be identified by gently crimping the eyelids with hemostats or with a dermatologic marker pen. B, The apex of the triangle or “wedge” to be resected is then marked in a similar manner. Usually the height of this triangle is approximately twice its base. C, The skin incision is made with a No. 15 Bard-Parker scalpel while the eyelid is supported by a Jaeger lid plate. D, The subcutis and conjunctiva are cut with straight Mayo or Stevens tenotomy scissors, so that the tissue wedge is completely resected. The method of closure is described in Figure 6-12.
PROMINENT NASAL FOLDS
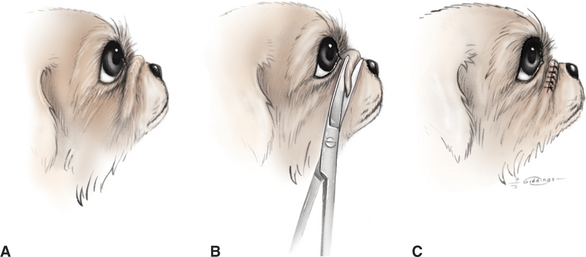
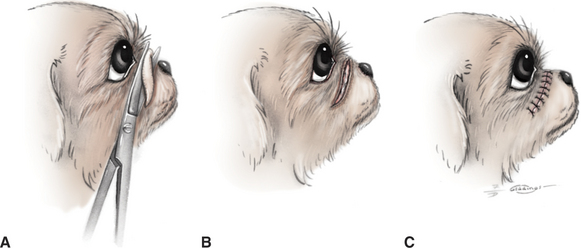
If nasal folds are causing keratitis, they should be removed either partially (Figure 6-13) or totally (Figure 6-14). In partial removal, only the medial portion of the fold is removed, where it touches the cornea, resulting in less alteration from the breed “norm” desired by some owners. The wound is closed with simple interrupted sutures of 4/0 silk placed 2 mm apart. In both methods the suture ends should be short enough to prevent corneal irritation. Sutures are removed 10 days later. Postoperatively, an Elizabethan collar is used. Nasal fold removal should be performed in conjunction with reconstructive medial canthoplasty when there is associated corneal drying, corneal exposure, and keratitis due to macropalpebral fissure and lagophthalmos or lower medial entropion (see later discussion of brachycephalic ocular syndrome).
DISORDERS OF THE CILIA
Normally positioned cilia emerge from the dermal side of the eyelid margin (Figure 6-15, A). The three common disorders in which aberrant cilia or hair cause corneoconjunctival irritation are as follows:
Clinical Signs of Cilia Disorders
All cilia disorders produce similar signs, as follows:
Treatment of Distichiasis
Cryoepilation
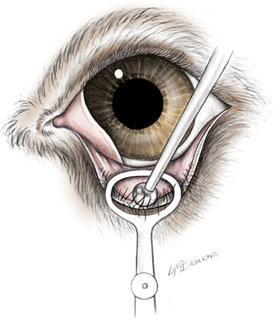
Cryoepilation takes advantage of the selective susceptibility of hair follicles to cold. A nitrous oxide or liquid nitrogen cryoprobe is applied to the conjunctiva overlying the meibomian glands that contain the offending cilia (Figure 6-17). The ice ball is observed as it advances over the line of gland openings on the eyelid margin. Two rapid freeze–slow thaw cycles are used. Following thawing of the second freeze, all visible cilia are manually epilated. Postoperatively, the eyelid swells and the meibomian glands undergo cryonecrosis. However, eyelid tissues other than the follicle are relatively spared. By 4 weeks, the treated meibomian glands have regenerated without cilia; however, new cilia may appear from untreated areas.
Failures with cryoepilation may be attributed to the following:
Treatment of Ectopic Cilia
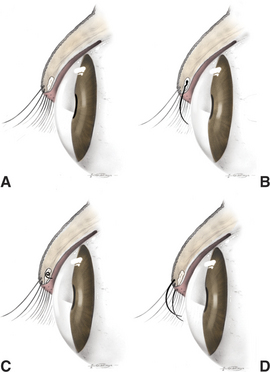
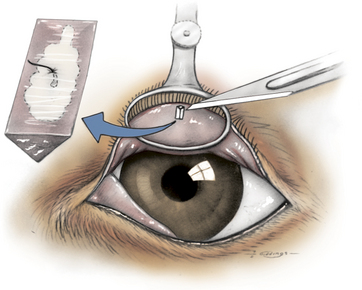
Ectopic cilia are treated with resection of the affected cilium and meibomian gland under magnification. An elliptical Desmarres chalazion clamp with screw lock is placed around the cilium for hemostasis, and the eyelid is everted. A block of tissue containing the offending follicle and meibomian gland is removed with a small (No. 65 Beaver) scalpel blade (Figure 6-18), leaving the eyelid margin intact. No sutures are placed. Digital pressure for several minutes is sufficient to control hemorrhage. A topical broad-spectrum antibiotic ointment is applied three times daily for 5 to 7 days postoperatively. If correctly performed, this technique is highly effective and is rarely associated with recurrence, although follicles may arise in the future from different sites.
Treatment of Trichiasis
Depending on location of the offending hairs, trichiasis is treated with any of the following:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


