Chapter 11 Exercise and stress testing
ELECTROCARDIOGRAPHY
Exercising electrocardiographic methods
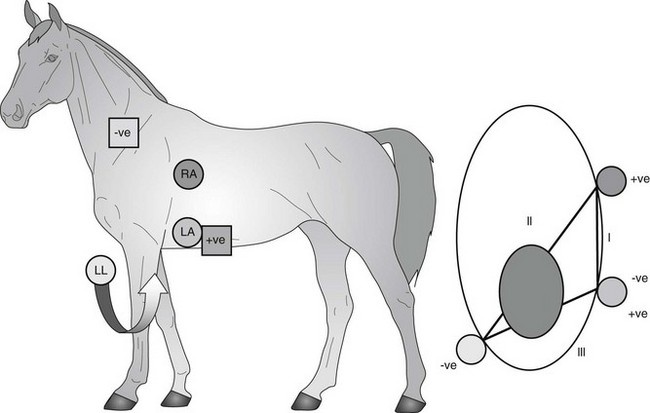
Electrocardiography (ECG) is the gold standard for definitively diagnosing rhythm disorders,1,2 and permits monitoring of the horse’s heart rate and rhythm during exercise. Continuous monitoring of the ECG can be accomplished with telemetry, with electrodes positioned in a modified base-apex configuration and attached to a transmitter that sends signals to a receiver.3,4 Electrodes can either be placed on the neck base and flank or positioned, under a surcingle, at the level of the sixth or seventh intercostal space (Fig. 11.1). The signal is then displayed on an oscilloscope, which can be digitized or printed to permanently record the ECG. These types of systems can be used in conjunction with various exercise tests that best mimic or exceed the usual level of exercise of the horse. This can include simply lungeing the horse, riding the horse on the flat or over jumps, or exercising it at high speed on a racetrack, training gallop or on a high-speed treadmill.
Although less desirable than telemetry, continuous 24-hour ambulatory ECG monitoring (see Chapter 10) can also be used to monitor heart rate and rhythm during exercise. The main disadvantage with Holter monitors is that they do not display the ECG in real time. However, in some situations, when the exercise area is beyond the range of a telemetry unit, they may be more appropriate to use. For example, if it is not practical to reproduce exercising conditions using a treadmill, arena or racetrack, such as may occur with dysrhythmias suspected during endurance exercise, a Holter monitor can be placed during a long distance ride. This allows the potential to re-create similar environmental conditions and stresses. Holter montitors can also be used to identify the presence of dysrhythmias in a 24-hour period that warrants assessment for dysrhythmias during exercise.
Heart rate
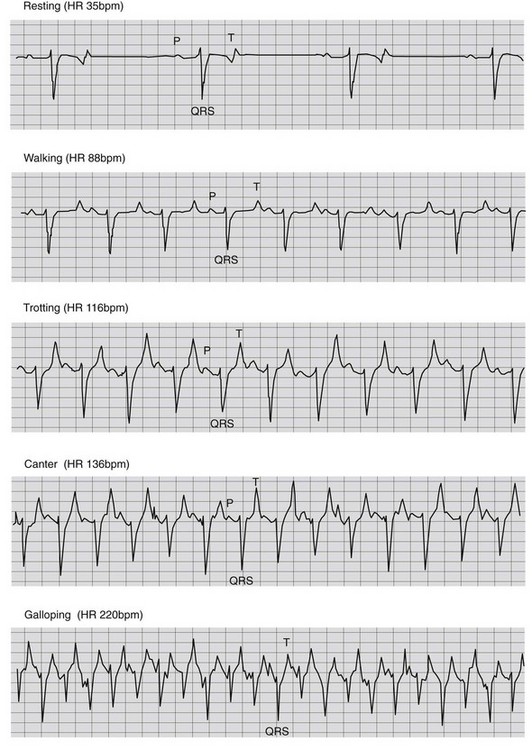
Monitoring the heart rate at different exercise intensities and as the horse recovers from exercise has been utilized to determine fitness and the presence of possible cardiac disease. A range of heart rates for various exercise intensities has been described, with an expected heart rate of 80–120 beats per minute (bpm) at the trot (nonracing), 120–150 bpm at the canter, 150–180 bpm at a hand gallop and >200 (200–240) bpm at maximum exercise intensity4 (Fig. 11.2). If the heart rate deviates from these ranges, cardiac disease or lack of fitness may be a cause; however, it is important to remember that noncardiac factors may play a role in determining heart rate, including pain, respiratory disease, dehydration, or environmental conditions such as high heat or humidity. These other causes must first be ruled out before attributing heart rate deviations to cardiac disease. These ranges are also useful to determine if the horse is capable of performing its expected workload. If a horse can attain the desired level of work before reaching its maximal heart rate, it should theoretically be able to maintain that intensity, barring other problems. If it reaches a maximal heart rate at low speeds or exertion, it is unlikely it will be able to perform more vigorously. ( AF, VSD)
AF, VSD)
Dysrhythmias associated with exercise
Monitoring for the presence of dysrhythmias is the most important benefit of performing an exercising ECG. Continuous monitoring of the heart rhythm during exercise is vital to the diagnosis of dysrhythmias that may impact performance, or potentially even result in collapse or death. ( AF) Paroxysmal atrial fibrillation (PAF) is an important cause of poor performance;5–7 however, it can be difficult to document because horses often convert to sinus rhythm before it is possible to complete a detailed electrocardiographic examination.6,8 Therefore, it may be difficult to confirm PAF in those horses in which an irregularly irregular rhythm is auscultated after fading or stopping in a race, unless an ECG is obtained at that time. However, the presence of frequent supraventricular premature depolarizations (SVPD) in a 24-hour period might support a tentative diagnosis of PAF in these situations. If numerous ventricular premature depolarizations (VPD) are observed in a 24-hour period, shortly after an exercise-associated dysrhythmia is auscultated, this may suggest that the dysrhythmia could have been ventricular in origin. (
AF) Paroxysmal atrial fibrillation (PAF) is an important cause of poor performance;5–7 however, it can be difficult to document because horses often convert to sinus rhythm before it is possible to complete a detailed electrocardiographic examination.6,8 Therefore, it may be difficult to confirm PAF in those horses in which an irregularly irregular rhythm is auscultated after fading or stopping in a race, unless an ECG is obtained at that time. However, the presence of frequent supraventricular premature depolarizations (SVPD) in a 24-hour period might support a tentative diagnosis of PAF in these situations. If numerous ventricular premature depolarizations (VPD) are observed in a 24-hour period, shortly after an exercise-associated dysrhythmia is auscultated, this may suggest that the dysrhythmia could have been ventricular in origin. ( AF)
AF)
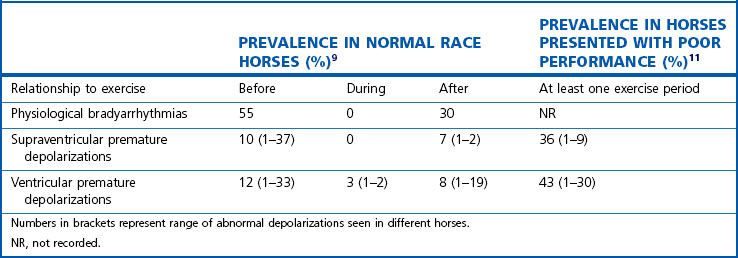
Horses have a high prevalence of dysrhythmias at rest that are vagally mediated and disappear with exercise. They may also have occasional premature depolarizations at rest; however, if they are infrequent, isolated and disappear with exercise they are unlikely to be of consequence (see Figs. 10.1 and 10.2). Conversely, horses may have a normal sinus rhythm at rest; however, this does not preclude them from developing dysrhythmias during peak exercise. That may impact performance. Cardiac dysrhythmias may be present before, during and after exercise in horses with no underlying cardiac disease and their interpretation can be difficult. A recent study examined the occurrence of dysrhythmias during warm-up, exercise and in the immediate post-exercise period in clinically healthy horses performing up to expectations9. In this study, isolated SVPD and VPD prior to exercise were a relatively common occurrence in these clinically normal horses. The etiology of these premature beats was unknown, although may relate to psychological factors. As many as 33 SVPD and 37 VPD were reported during that time period9. (Table 11.1).
Table 11.1 Prevalence of cardiac arrhythmias as detected using ambulatory recordings around exercise in normal race horses (n = 99) and in racehorses presented for assessment of poor performance (n = 88)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


