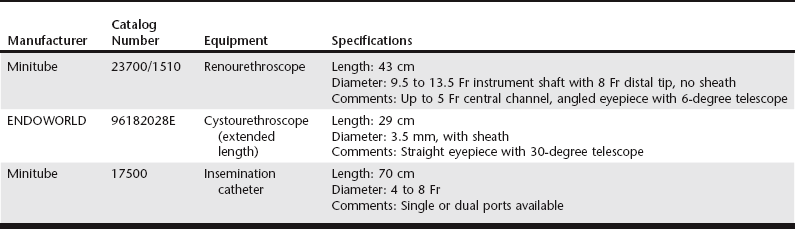
Chapter 206 Dr. Marion Wilson developed the noninvasive TCI technique using a rigid endoscope specifically to deposit frozen-thawed semen into the uterus of the bitch (Wilson, 2001). Research of this technique resulted in identification of several features relating to the anatomy of the canine reproductive tract. These points are relevant to endoscopic TCI and are considered first, followed by a description of relevant procedures for TCI. The endoscope initially identified as meeting the criteria with regard to length and diameter was a rigid, extended length cystourethroscope (Table 206-1). An 8 Fr urinary catheter is used for insemination in the majority of bitches using this endoscope, although a 6 Fr gauge sometimes is required in small or maiden bitches. More recently, a longer (43 cm) and thinner (graduated 9.5 Fr to 13.5 Fr) rigid renourethroscope has been developed for the TCI procedure in bitches. A specially designed 70 cm × 5 Fr catheter (Minitube) with removable stylet is used for insemination of most bitches. Occasionally a 4 Fr catheter is required in small or toy breeds that can have a smaller os and cervical canal. A specially designed platform is used to restrain the bitch in the standing position. The platform provides a tie point to the dog’s collar and an abdominal support to restrict sideways movement and discourage any attempt to sit (Figure 206-1). A hydraulic chair together with a hydraulic table for the platform ensures the optimum position of the bitch relative to the operator during the procedure. This is important particularly when the endoscope is used without a camera. Bitches in estrus exhibiting standing behavior show excellent tolerance to the technique and sedation is rarely necessary.
Endoscopic Transcervical Insemination
Equipment
< div class='tao-gold-member'>
Endoscopic Transcervical Insemination

Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


