Chapter 9 Endoscopic Placement of Gastrostomy and Jejunostomy Tubes
Indications
PEG-J tubes have been used less commonly in veterinary medicine. Common indications for the use of jejunostomy tubes include conditions predisposing animals to aspiration (e.g., regurgitation, vomiting, and significant obtundation), functional or mechanical obstructions (e.g., gastric stasis or atony, pyloric obstruction, and proximal small intestinal obstruction), significant gastric disease or gastrectomy, and pancreatitis. The use of gastrojejunostomy tubes in patients with pyloric outflow tract obstruction or small intestinal obstruction is dependent on the ability to successfully advance the jejunostomy tube. Endoscopic placement of nasojejunostomy tubes has been described; it may be a useful alternative for patients at high risk of stoma dehiscence that would otherwise benefit from jejunal feeding.
Megaesophagus and PEG or PEG-J Tubes
The use of PEG tubes in patients with megaesophagus remains controversial. In several recent reports, PEG tubes were successfully utilized to manage patients with megaesophagus that were unable to independently maintain adequate caloric intake. Three of four dogs with megaesophagus secondary to tiger snake envenomation received PEG tube placement as part of their case management.1 Two of these dogs survived to discharge and continued to be fed via tube until the megaesophagus resolved (30 and 36 days). Gastrostomy tube feedings were also successfully utilized in treatment of six other dogs with megaesophagus (etiology not stated), and a cat with megaesophagus after diaphragmatic repair.2,3 Megaesophagus was classified as idiopathic in three of four dogs receiving replacement low-profile gastrostomy tubes in one study.4 None of these dogs died or was euthanized as a result of complications from tube feeding. These dogs were maintained with the use of replacement low-profile tubes for 31, 1017, 723, and 1020 days. The first two dogs were still alive at the time the study was published; the other two died from non-tube–related causes.
Advantages of PEG Tubes
Disadvantages of PEG Tubes
Advantages of PEG-J Tubes
Disadvantages of PEG-J Tubes
Equipment
Gastrostomy Tubes
Placement Style
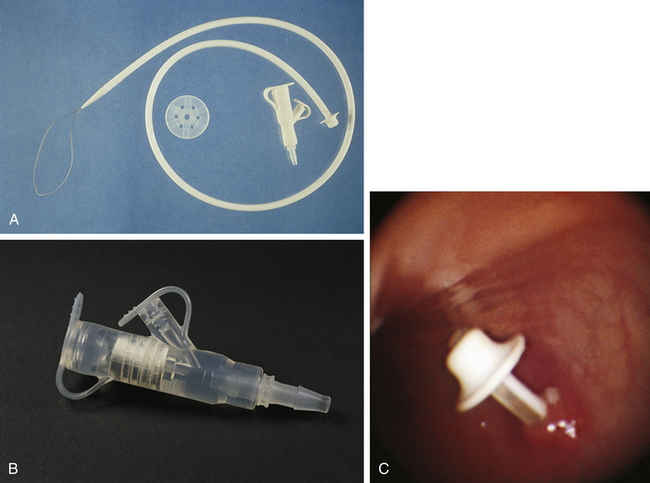
PEG tubes are generally designed for one of two placement techniques (pull versus push). The majority of PEG tubes are initially placed by the pull method. Tubes installed with the use of the pull method are pulled through the mouth into the stomach with a long suture and then outward through the gastric and body walls. The tube has, or is modified to have, a tapered end with an attachment mechanism or loop so it can be smoothly pulled through the gastric wall (Figure 9-1). With the push method, the tube is pushed over a guidewire from the mouth into the stomach and out through the body wall. The proximal end of the tube is tapered to push across the stomach and body walls and is fenestrated for passage of the guidewire.
Anatomy
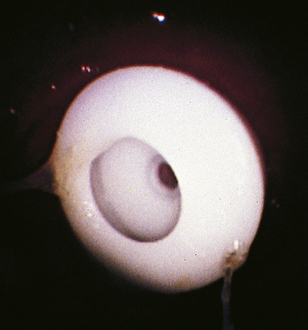
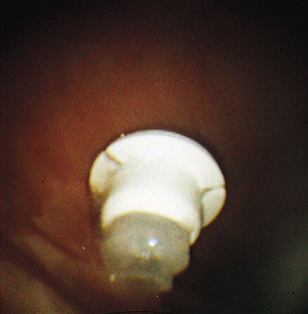
Retention of the PEG tube in the stomach is dependent on the tube’s internal bumper or retention disk. The anatomy of the bumper varies by manufacturer and placement technique (Figures 9-2 through 9-4). Bumpers are designed to balance the risk of accidental dislodgement against the risk of gastric necrosis and the invasiveness of tube removal or replacement. Bumpers that offer a decreased risk of accidental dislodgement generally require endoscopic removal, whereas those that may be removed through the body wall by applying traction with or without the use of a stylet are more susceptible to premature removal. When selecting a PEG tube for placement, the clinician must weigh the patient’s temperament and the anticipated need for tube removal or replacement against the patient’s size, anesthetic risk, and the client’s finances.

Sizes
Tubes with luminal diameters of 18F to 24F are commonly utilized in dogs and cats. Clinicians are encouraged to use larger diameter tubes whenever possible, particularly if PEG-J placement or replacement with a low-profile gastrostomy button is desired or anticipated. When using mushroom-tip or Pezzer catheters, it is particularly important to select a large-bore tube with a rigid tip to minimize the risk of premature dislodgement.
Additional Materials
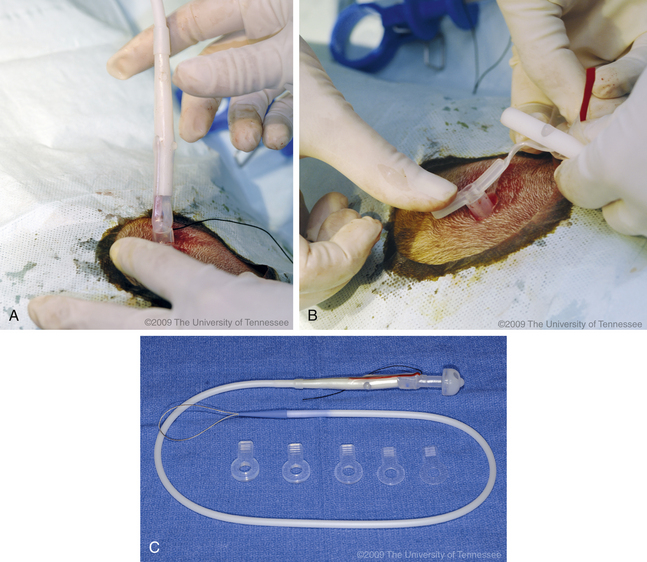
Components of a homemade kit are displayed in Figure 9-5. The majority of these materials are included in commercial feeding tube kits. See Box 9-1 for a checklist of materials necessary for PEG tube placement.

BOX 9-1 Equipment Checklist for Percutaneous Endoscopic Gastrostomy (PEG) Tube Placement by the Pull Method
Low-Profile Gastrostomy Tubes
Low-profile gastrostomy tubes or buttons (PEG-B) offer a number of advantages over traditional tubes. The compact and self-retaining designs (Figure 9-6) generally eliminate the need for external dressings and retention sutures, which improves patient tolerance, aesthetics, and ease of management. The presence of a one-way valve minimizes reflux of food during administration, while alternate attachments facilitate gastric sampling and suction.

One-Step Gastrostomy Tubes
Although low-profile gastrostomy tubes have historically been used as replacement tubes, several commercial one-step low-profile gastrostomy button (OSB) kits (Figure 9-7) are available for primary placement. Because of their aesthetic benefits, large luminal diameters, and ease of use, OSBs are increasingly being utilized as the tube of choice in human medicine. Initially, placement of OSBs was associated with a high prevalence of peri-PEG cellulitis, button migration, and secondary peritonitis. These complications have been decreased with changes in tube design and may be minimized further through careful selection of the appropriate OSB shaft length and creation of an adequately large skin incision. In a recent study in children, equivalent complication rates were noted for OSBs and traditional PEG tubes, but tube life and feeding tolerance were much higher in the OSB group.7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


