Chapter 21 Arthroscopy
Patient Contraindications
There are few contraindications specifically for arthroscopic surgery. Perhaps the most common contraindication would be animals or joints that are simply too small to allow examination. When a 1.9-mm arthroscope is used, dogs as small as 12- to 13-kg body weight may be scoped, but instrumentation of joints in very small dogs and cats may be difficult or impossible. Dogs with severe arthritis and poor joint range of motion may present a challenge to the arthroscopist, but these severely degenerative joints are not a contraindication. Besides small size of the animal, the only other contraindications would be general ones that apply to any surgery, such as animals being poor anesthetic candidates or having severe systemic diseases rendering their joint problems irrelevant.
Equipment for Small Animal Arthroscopy
Arthroscopes
The initial instrument that is considered is the arthroscope itself. Arthroscopes are surgical telescopes that allow visualization of the joint. These scopes are rigid tubes with lenses on the ends and fiberoptic bundles in the tube that allow transmission of the image and light. Arthroscopes are available in several diameters including 4.0, 2.7, 2.4, and 1.9 mm (Figure 21-1). The most commonly used endoscope in small animal orthopedics is the 2.7-mm arthroscope. The 2.4-mm scope is very similar, and the 1.9-mm scope is useful in smaller joints such as the carpus or tarsus. The 4.0-mm scope is too large for most dogs and is rarely used in companion animals. In addition to varying diameters, several lengths and viewing angles are available for arthroscopes. Most veterinary arthroscopists use a shorter scope (12 cm or less in length), although scopes are available up to 18 cm. Viewing angles of 0, 30, and 70 degrees have been used in the past, but the 30-degree arthroscope is almost exclusively used by veterinary arthroscopists. Even though arthroscopes have an eyepiece for direct viewing, all modern arthroscopy is performed with the use of a video arthroscope. The final feature of all arthroscopes is a post for attaching the light cable.
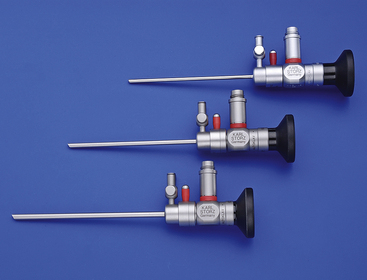
Figure 21-1 Commonly used arthroscopes for small animal surgery include the 2.7-, 2.4-, and 1.9-mm arthroscopes.
(Photo courtesy of Karl Storz GmbH & Co. KG, Tuttlingen, Germany.)
Video Camera and Control Unit, Light Sources, and Monitor
The monitor is the screen that is used to visualize the joint. Most modern monitors are high-definition flat screen monitors that give excellent picture quality. Monitor size varies considerably, but the rule of thumb is to purchase the largest monitor that fits your arthroscopy cart and your budget. A 21-inch or larger monitor is ideal because it allows the arthroscopy cart to be backed away from the surgical table as much as possible. The operating table area gets very crowded with all of the equipment necessary to perform the procedure, and the farther the arthroscopy cart is from the table, the more room is left for the surgeon and assistant to work.
Fluid Management
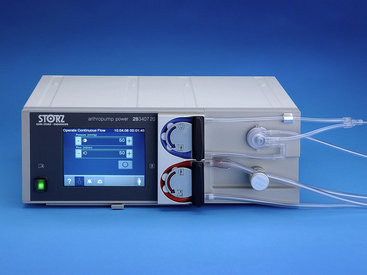
The ideal way to deliver fluid to the joint is to use a mechanical arthroscopy pump (Figure 21-2). Several manufacturers market these pumps, and most use either an impeller or a roller pump to control fluid flow rate. A transducer built into the fluid line is used to precisely control pressure within the joint. The pumps work well, and fluid extravasation is minimized through optimal fluid management. For most arthroscopic procedures, a high flow setting is used with a modest pressure. Typically, pressures within the joint are set at 25 to 40 mm Hg. If bleeding from the joint capsule is a problem or the joint is not distending well, higher pressures can be used but rarely exceed 60 mm Hg. When choosing an arthroscopy pump to purchase, one should investigate the cost of the pump along with the cost of the tubing to determine whether the tubing can be used on more than one case or can be resterilized. Single-use tubing that cannot be reused may be prohibitively expensive.
Shavers
A power shaver is an important part of any arthroscopy setup (Figure 21-3). The power shaver is a motorized power tool that allows the rapid and precise removal of bone, cartilage, and soft tissue. The essential components of most power shaver units are the electronic control box, a handpiece and bit, and the foot pedal. The power shaver may be controlled with the use of a hand control or a foot control, but most surgeons prefer a foot control. The control box contains the electrical apparatus and controls for revolutions per minute of the handpiece. The handpiece is the motor and couples to interchangeable bits for different jobs, and the foot pedal is a variable speed controller that also allows the bit to rotate forward or backward or to oscillate. The speed of the handpiece is generally set to 1500 to 2500 rpm for most small animal procedures. Bits are cannulated so that debris that is cut is immediately removed from the joint by surgical suction that is coupled to the handpiece. Bits are a tube within a tube in which the inner tube rotates. The outer tube is a tissue guard that serves to protect the soft tissue. There is a defect on the side or end of the outer tube that exposes the blade or burr that does the cutting. Many types of bits are available, but the most useful for small animal arthroscopy are aggressive cutting blades that are 2.5 to 4.0 mm in diameter. Burr bits are also helpful and can be obtained in the same size range.

Hand Instruments
The first hand instrument necessary is a probe (Figure 21-4). This is a straight stainless steel rod with a 90-degree bend at the end so that it forms a small hook. This instrument is used to manipulate pieces of bone and cartilage, retract soft tissue, and check the integrity of articular tissues. A small probe is best, and perhaps the most useful is a temporomandibular joint (TMJ) probe designed for use in the TMJ of humans. It is a nice size probe and easily fits through a 2.9-mm cannula. Some probes have alternating color bands so that the surgeon can get an idea of dimension when exploring joints or measuring lesions.

Figure 21-4 Arthroscopic hand instruments include probes and graspers of various types and sizes.
(Photo courtesy of Karl Storz GmbH & Co. KG, Tuttlingen, Germany.)
Arthroscopic scissors are required for some procedures, such as trimming meniscal tears in dogs. They come in a variety of sizes, but the most useful have relatively short blades and are 2.0 to 3.0 mm in diameter.



