Chapter 14
Endoscope-Assisted and Endoscopic Surgery
In human medicine, endosurgery has been credited with numerous advantages over traditional open procedures, including reductions in pain, operating time, hospital stay, and convalescence period.1,2 While such advantages may be less easily quantified or published in veterinary medicine, over the past decade there have, nevertheless, been considerable advances in minimally invasive endosurgery of animals, including reptiles.3–6 Indeed, considering that most reptiles weigh less than a few kilograms, the development of minimally invasive endosurgery would seem a logical evolution in their surgical care, particularly given the hindrances of the chelonian shell.7
Endosurgical Equipment
In addition to a telescope, one or more independent instruments must be introduced when the endoscopist operates inside a reptilian coelom.8 These instruments and the cannulae through which they pass are grouped into various size classes that are often color-coded. For example, 2-mm instruments are used in conjunction with 2.5-mm cannulae, 3-mm instruments with 3.5-mm cannulae, and 5-mm instruments with 6-mm cannulae (Figure 14-1). In addition, the 2.7-mm telescope housed within a 3.5-mm protection sheath will pass through a 3.9-mm cannula. A listing of available equipment is provided in Table 14-1.8
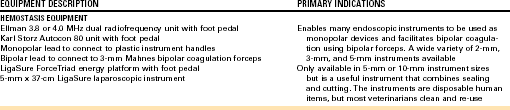
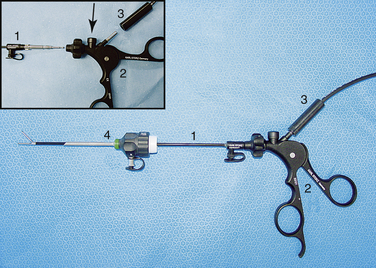
FIGURE 14-1 Human pediatric 3-mm laparoscopy equipment. A 3-mm instrument (1) attached to a standard ClickLine handle (2). The instrument, attached to a radiosurgery unit via a connector on the handle (3), has been inserted through a 3.5-mm graphite/plastic cannula (4). Inset, Instrument (1) and handle (2) can be quickly exchanged by pressing on the release button (arrow). The radiosurgical connection is also shown (3). (Courtesy Dr. Stephen J. Divers, University of Georgia, Athens, Ga.)
Cannulae and Trocars
Cannulae are used to provide additional access ports (Figure 14-2). They are of surgical steel or graphite/plastic construction and have internal leaflet valves and optional insufflation stopcocks for CO2 delivery. These valves are designed to prevent loss of gas during insufflation. Insufflation stopcocks are optional, but at least one is required for the attachvment of the insufflation line. The metal cannulae are more robust and heavier and therefore are used only for the animals weighing more than 10 kg (i.e., 6-mm cannulae for 5-mm instruments). The plastic/graphite models are extremely light and ideally suited to most small reptiles (i.e., 2.5-mm and 3.5-mm cannulae for 2-mm and 3-mm instruments, respectively). Most cannulae are used in conjunction with trocars. A trocar is a solid, often sharp and pointed, metal rod that is inserted into the cannula to assist with placement. Most are sharp to facilitate perforation of the body wall when axial and penetrative force is applied.
FIGURE 14-2 Cannulae and trocars. A, A 2.7-mm telescope within a 3.5-mm protection sheath (1) inserted through a 3.9-mm × 10-cm graphite/plastic cannula with insufflation side port (2). B, A 3.9-mm × 10-cm graphite/plastic cannula disassembled to illustrate the graphite cannula (1), leaflet valve (2), screw cap (3), and instrument seal (4). C, A 3.9-mm × 10-cm graphite/plastic cannula with insufflation side port (1) and 3.5-mm × 10-cm threaded cannula with insufflation side port and trocar inserted (2). The 3.9-mm cannula can accommodate the 2.7-mm telescope housed in a 3.5-mm protection sheath, whereas the 3.5-mm cannula can accommodate 3-mm instruments. The threaded design resists dislodgement in small exotic species. D, Ternamian EndoTip cannulae; 6-mm × 15-cm with insufflation side port and multifunctional valve (1) and 6-mm × 10.5-cm cannula with silicone leaflet valve. These metal cannulae are far heavier and best restricted to animals weighing more than 10 kg. (Courtesy Dr. Stephen J. Divers, University of Georgia, Athens, Ga.)
The threaded cannula (e.g., EndoTip) is a recent improvement that has an external screw thread to enable gradual advancement by rotation (see Figure 13-2 C, D).9 These threaded cannulae are available in 3-mm, 3.9-mm, and 5-mm sizes and do not require a trocar or much axial penetrative force for insertion. A telescope positioned inside the cannula provides a magnified view during entry into the coelom. As the cannula is advanced, the fascia and then the muscle fibers spread radially and are transposed onto the cannula’s outer thread. The thin coelomic membrane is transilluminated so that viscera, vessels, and/or adhesions are visualized before entry into the coelom (Figure 14-3). The risks of iatrogenic visceral damage are therefore greatly reduced. In addition, the threads also provide greater security in that such cannulae are less likely to be dislodged.
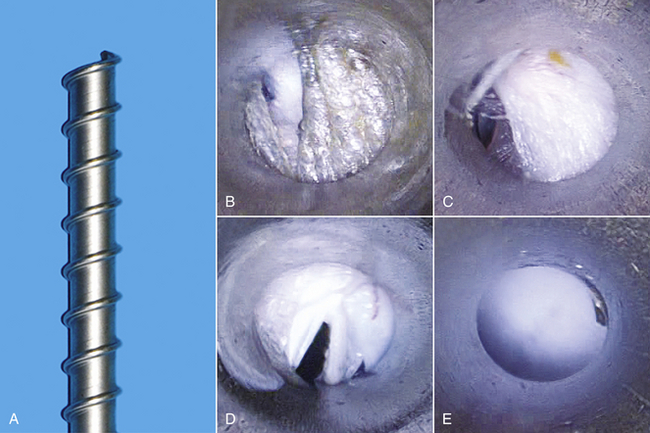
FIGURE 14-3 A, A terminal end of a 6-mm threaded cannula. Screwed entry of the threaded cannula through an initial skin incision (B), subcutaneous tissue (C), and finally the coelomic membrane (D) before entering the coelomic cavity (E). (Courtesy Dr. Stephen J. Divers, University of Georgia, Athens, Ga.)
Instruments and Handles
At least one, generally two, and rarely three instruments are inserted through cannulae and into the endoscopic field of view. Instruments must be triangulated to bring the instrument tips together (convergence) and enable surgery within the reptilian coelom. A large assortment of 5-mm instruments are available; they were initially developed for humans but are equally applicable for animals more than 10 kg. However, it was not until the development of human pediatric laparoscopy that smaller 2-mm and 3-mm instruments became available and multiple-entry endosurgery became feasible in smaller animals.10
Currently, 2-mm instruments are limited to Babcock forceps, dissecting forceps, and scissors. A greater selection of 3-mm instruments are available, including a variety of dissecting forceps, grasping forceps, scissors, biopsy forceps, and palpation and irrigation probes (Figure 14-4). All these instruments have a standard attachment that enables them to be used interchangeably with a selection of ClickLine handles (Figure 14-5). Handles are of plastic or metal construction and may have a radiosurgical connection that enables scissors or forceps to be used as monopolar devices. An optional hemostat, Mahnes, or disengageable-style racket mechanism is available to maintain firm hold of tissue, even if the endoscopist releases the grip on the handle (see Figure 14-5, B, C, E).
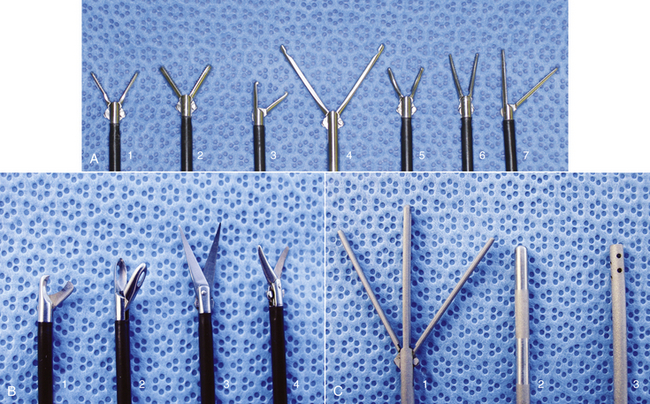
FIGURE 14-4 A selection of 3-mm instruments. A, Forceps: fenestrated atraumatic grasping forceps (1), Reddick-Olsen dissecting forceps (2), small Babcock forceps (3), large Babcock forceps (4), short curved Kelly dissecting and grasping forceps (5), long curved Kelly dissecting and grasping forceps (6), and atraumatic dissecting and grasping forceps with single-action jaws (7). B, Scissors and biopsy instruments: microhook scissors with single action jaws (1), Blakesley dissecting and biopsy forceps (2), scissors with long sharp curved double action jaws (3), and scissors with serrated curved double action jaws (4). C, Probes: distendable palpation probe (1), palpation probe with centimeter markings (2), and irrigation and suction cannula (3). (Courtesy Dr. Stephen J. Divers, University of Georgia, Athens, Ga.)
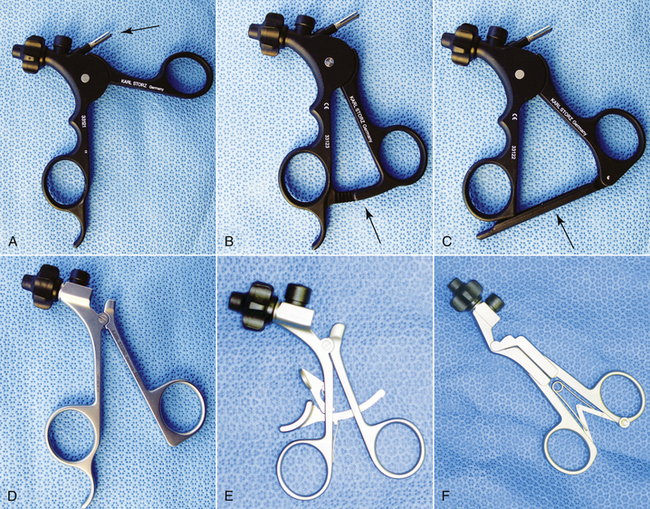
FIGURE 14-5 Endoscopy instrument handles. A, Plastic handle (without racket) with radiosurgery connector (arrow). B, Plastic handle with hemostat-style racket (arrow). C, Plastic handle with Mahnes-style racket (arrow). D, Metal handle without racket or radiosurgery connection. E, Metal handle with disengageable racket but no radiosurgical connection. F, Metal Y-handle with spring action. (Courtesy Dr. Stephen J. Divers, University of Georgia, Athens, Ga.)
Surgical Devices and Hemostasis
Effective and safe performance of endoscopic surgery requires accurate hemostasis because the mere act of clamping a bleeding vessel or dabbing with gauze may be impossible. Radiosurgery and laser surgical devices have become available and can facilitate internal incision and debridément while hemorrhaging is controlled. Diode lasers (e.g., AccuVet Lumenis Inc., Norwood, Mass) are, by design, able to pass through flexible fiberoptic probes that can be inserted through instrument channels or cannulae (Figure 14-6).11,12 A variety of diode laser probes are available; however, 400 to 600 μm conical or flat tips at 2 to 10 watts are generally most useful (SurgiMedics Inc., The Woodlands, Tex). Until recently, CO2 lasers (AccuVet Lumenis Inc.) could not be used via endoscopic instrument channels because of the inflexible nature of the ceramic delivery probes. The development of a long semirigid probe (AccuVet Lumenis Inc.), however, has enabled the use of the CO2 laser via the 1.7-mm instrument channel of the 4.8-mm operating sheath. Nonetheless, although it is functional, it is rather cumbersome (Figure 14-7). Probably the most versatile device, especially when using 3-mm or smaller instrumentation systems, is a radiosurgery unit because a wide variety of tools are available for use with foot-pedal activated radiosurgery 3.8 and 4.0 MHz Surgitron, (Ellman International Inc., Oceanside, NY) (Figure 14-8) and electrocautery (Autocon 80, Karl Storz Veterinary Endoscopy, Goleta, Calif) units.13 The most useful includes various needle electrodes (Ellman International Inc), bipolar forceps, and a retractable polypectomy snare (Karl Storz Veterinary Endoscopy America Inc., Goleta, Calif). The degree of radiosurgical power required during endosurgery varies with operating conditions and the instrument being used, but because of the microsurgical nature of most endosurgical procedures, lower settings are generally required compared with open surgery. Considerable growth in endoscopic radiosurgery has led to the availability of a large number of monopolar and bipolar devices. One particularly favored device among human and veterinary endosurgeons is the LigaSure ForceTriad (Covidien, Boulder, Colo) (Figure 14-9). This system detects the thickness (by measuring the electrical impedance) of tissue to be coagulated and automatically defines the amount of energy required and the delivering time. An acoustic signal informs the surgeon when the vessel obliteration is complete and its division is possible. Unfortunately, endoscopic handpieces smaller than 5 mm are not yet available, limiting its usefulness to 5-mm systems and the largest of reptiles (Figure 14-10).
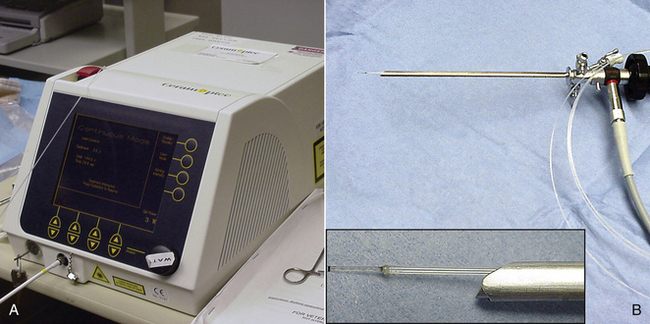
FIGURE 14-6 A, A 980-μm diode laser unit. B, A 600-μm diode laser fiber inserted down the instrument channel of the 4.8-mm operating sheath and emanating from the terminal end of the sheath in front of the terminal telescope lens (inset). (Courtesy Dr. Stephen J. Divers, University of Georgia, Athens, Ga.)

FIGURE 14-7 A, Elongated ceramic CO2 laser tip inserted down the instrument channel of the 4.8-mm operating sheath. B, The same ceramic tip alongside the sheath. (Courtesy Dr. Stephen J. Divers, University of Georgia, Athens, Ga.)
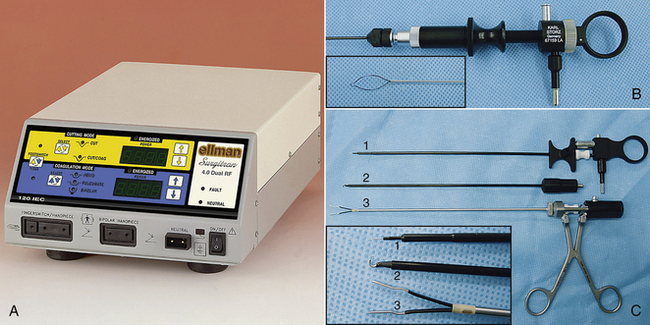
FIGURE 14-8 A, A 4.0 MHz dual frequency radiosurgery unit (4.0 MHz Surgitron, Ellman International, Inc.). B, Polypectomy snare handpiece with extended end shown (inset). C, Various radiosurgical endoscopic devices; retractable needle (1), dissecting hook (2), and bipolar forceps (3). Close-up of instrument ends also shown (inset) (Karl Storz Veterinary Endoscopy, Goleta, Calif). (Courtesy Dr. Stephen J. Divers, University of Georgia, Athens, Ga.)

FIGURE 14-9 The LigaSure vessel sealing system and a disposable 5-mm endoscopic sealing and cutting instrument. (Courtesy Dr. Stephen J. Divers, University of Georgia, Athens, Ga.)

FIGURE 14-10 A LigaSure Atlas handpiece (Covidien, Mansfield, Mass). This 10-mm instrument has a working length of 20 cm and is capable of sealing and transecting vessels up to 7 mm in size. The smallest diameter endoscopic instrument currently available is 5 mm, restricting this device to the largest of reptiles. (© University of Georgia Research Foundation, Inc.)
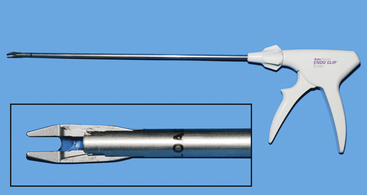
Another useful item from human and domestic animal laparoscopy is the endoscopic vascular clip applicator (Figure 14-11). These devices contain a cartridge of clips that can be rapidly employed without having to remove the instrument from the patient and reload. Again, the smallest available size is 5 mm, which restricts their use to the largest reptiles.
Endoscopy Tables
In human and domestic animal endosurgery, tilting tables are used to modify patient positioning and create advantageous organ displacement during surgery. Most of the table-mounted configurations used in veterinary medicine are designed for mammals and are incompatible with most reptiles. In addition, joystick-controlled tilting surgery tables (Figure 14-12) are helpful but expensive and likely to be limited to teaching hospitals and other major referral institutions. Most practitioners can probably achieve similar positioning, albeit with less intraoperative versatility, by using towels, sandbags, vacuum pads, tape, and various other positioning aids (Figure 14-13).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


