Chapter 159 Electrical and Lightning Injuries
INTRODUCTION
Electrocution may occur by contact with high-voltage or low-voltage electrical sources or by a lightning strike. It is generally accepted that chewing through household electrical cords is the most common cause of electrocution in dogs and cats. From 1968 to 2003, a database from several institutions* recorded that 280 dogs and 92 cats sustained electrical injuries. Of these, 54 dogs and 26 cats had chewed electrical cords, and 4 dogs and no cats were identified as having been struck by lightning. It is likely that many of the unspecified electrocutions were low-voltage injuries from chewing household electrical cords.
PREDISPOSITION TO ELECTRICAL INJURY
Young dogs and cats are the most common victims of electrical injury because they are more likely to chew on electrical cords than are older animals. The average age of dogs with electrical injury has been reported to be 3.5 months (range, 5 weeks to 1.5 years; n = 29); the range of age for seven cats was reported to be 2 months to 2 years.1 From 1968 to 2003, a database collected in several institutions* revealed that the most common age range for electrical injuries was 2 to 12 months; 186 of 280 (66%) dogs and 44 of 92 (48%) cats with electrical injuries and 38 of 54 (70%) dogs and 12 of 26 (46%) cats that sustained electrical injury from chewing electric cords were 2 to 12 months old. Seasonal predisposition is generally accepted, but there is some difference in opinion as to what time of year most injuries are seen. Holiday seasons characterized by use of decorative lights (Halloween, Christmas) certainly pose electrical risks,4 but one study reported that 79% of canine cases occurred during the 6 months from March through August.1
CLINICAL FINDINGS
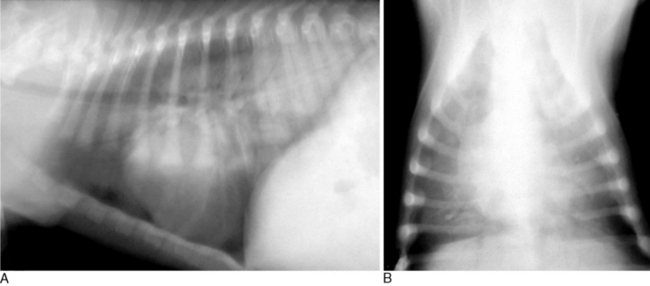
Causes of respiratory distress include facial or nasopharyngeal edema, diaphragmatic tetany, and neurogenic pulmonary edema. Neurogenic pulmonary edema is a form of noncardiogenic pulmonary edema in which central nervous system (CNS) insult results in massive sympathetic outflow that causes pronounced vasoconstriction and systemic hypertension. As a consequence, there is marked elevation of left ventricular afterload and decreased left ventricular stroke volume, which causes blood to accumulate in the pulmonary circulation, resulting in increased pulmonary capillary pressure and subsequent edema.9 The typical radiographic pattern is alveolar infiltration of the caudodorsal quadrant (Figure 159-1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


