CHAPTER 53 Disorders of the Guttural Pouch
The guttural pouches are outpouchings of the auditory tubes that connect the pharynx to the middle portion of the ear canals. Outpouchings of the auditory tubes are unique to horses and other equids, tapirs, hydraxes, some rhinoceros, some bats, and the South American forest mouse. The auditory tube outpouchings of the adult horse are the largest of any species, with each having a capacity of approximately 475 mL. Functions that have been proposed for the guttural pouches include equilibration of pressure across the tympanic membranes, resonating chambers for vocalization, and a role in cooling blood circulating to the brain.
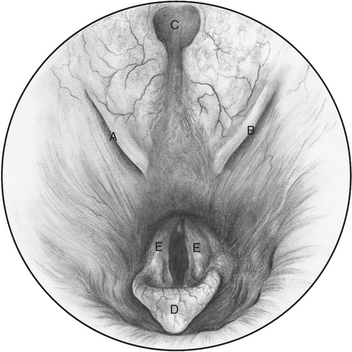
Guttural pouch disorders are related to the anatomic makeup of the pouches and their associations with surrounding tissues. Each pouch communicates with the pharynx through the rostral portion of the respective auditory tubes. The rostral portions of the auditory tubes are 2 to 3 cm long and funnel shaped, with the large end of the funnel opening into the pharynx. The pharyngeal openings are located on the dorsolateral aspects of the pharynx and are identified as oblique slits lying rostral and ventral to the pharyngeal recess. The medial wall of each opening is composed of a fibrocartilage flap oriented in a rostrodorsal-to-caudoventral direction (Figure 53-1).
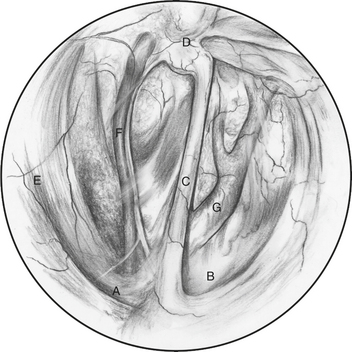
The guttural pouches are lined with pseudostratified ciliated epithelium containing goblet cells. The floor of each pouch is reflected over the ipsilateral stylohyoid bone, partially dividing the pouches into larger medial and smaller lateral compartments (Figure 53-2). The stylohyoid bones travel in a rostroventral to a caudodorsal direction to their temporohyoid articulations. The internal carotid artery; cranial cervical ganglion; cervical sympathetic trunk; and glossopharyngeal, vagus, spinal accessory, and hypoglossal nerves all course along the caudal wall of the medial guttural pouch compartment. The external carotid artery, cranial branch of the laryngeal nerve, pharyngeal branch of the vagus nerve, and retropharyngeal lymph nodes lie beneath the floor of the medial compartment. The external carotid artery travels from the medial compartment ventral to the stylohyoid bone and into the lateral compartment, where it gives off the caudal auricular and superficial temporal arteries and continues as the maxillary artery along the lateral dorsal wall of the lateral compartment. The facial and vestibulocochlear nerves course in close proximity to the lateral aspect of the temporohyoid joint. The right and left guttural pouches do not communicate with each other. They are separated by the rectus capitus ventralis and longus capitus muscles dorsally and meet ventrally to form a thin median septum.
GUTTURAL POUCH MYCOSIS
The characteristic lesion of guttural pouch mycosis, a fungal plaque, appears as a diphtheritic membrane, irregular in contour and closely attached to the underlying tissue. The plaque can be brown, green, white, black, or other colors and can range in size from a discrete nodule of a few millimeters to an expansive lesion covering a large portion of the guttural pouch. Fungal mycelia, a variety of bacteria, cell debris, and necrotic tissue make up the diphtheritic membrane. Several fungi have been identified in clinical lesions, with the most common being Aspergillus spp. Microscopically, fungal elements can be seen invading the underlying tissues including arteries and nerves. Moderate to severe local inflammation surrounding the lesions is common. Why or how the fungal infection begins is unknown.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


