Chapter 10. Diseases of the Lens
CHAPTER CONTENTS
Normal anatomy323
Lens protein breakdown or lens capsule rupture and its significance in inflammatory eye disease330
The lens epithelium and its role in disease after lens capsule rupture337
Lens luxation339
Subluxation 339
Anterior luxation 339
Posterior luxation 339
Detecting pre-existing lens luxation in the enucleated globe 339
Vision-threatening consequences of lens luxation 339
Causes of secondary lens luxation include 341
Breed-related zonular ligament dysplasia as a risk factor for canine primary lens luxation 341
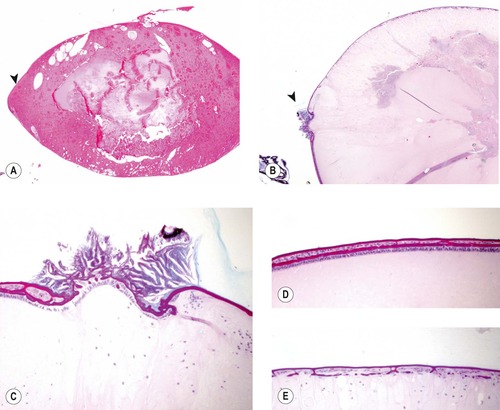
NORMAL ANATOMY (Fig. 10.1)
• The lens has only one cell type, the lens epithelial cell
• At all stages of lens development, except embryonic, normal lens epithelial cells are only present anteriorly, where they form a monolayer of cuboidal epithelium (Chapter 3 provides a more detailed discussion of lens development)
• At the lens equator, the lens epithelial cell elongates, rotates and is pushed inward. The cell then continues to elongate until the anterior and posterior tips of each lens fiber reach opposite poles of the lens. The fully differentiated lens fiber cells lose their nuclei and become compacted towards the center of the lens, as new fibers continue to form throughout life
• The lens is surrounded by a thick capsule which represents the basement membrane of the lens epithelium. Throughout life, the anterior lens capsule continues to thicken while the posterior capsule remains thin, since there are no lens epithelial cells at the posterior pole
• In mammals, the lens is held in place on the anterior vitreous face by a combination of the gentle pressure exerted from behind by the vitreous body, and the tension of zonular ligaments that suspend the lens circumferentially. These zonules are secreted by the ciliary epithelium and insert in a crossover pattern onto the equatorial lens capsule.
Comparative Comments
• The lens is a simple structure histologically and in the human generally conforms to the description given for the lens in other species
• The remarkable complexity of the lens is hidden at the molecular and functional levels.
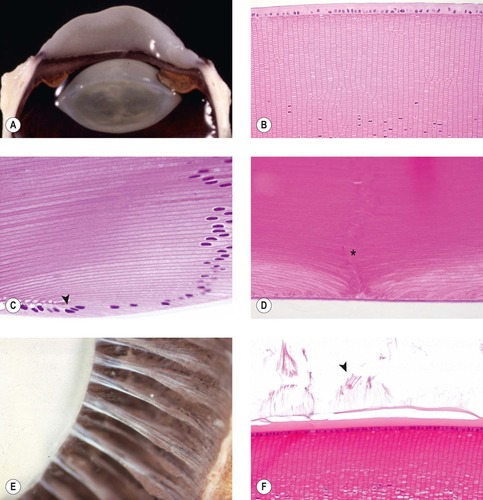 |
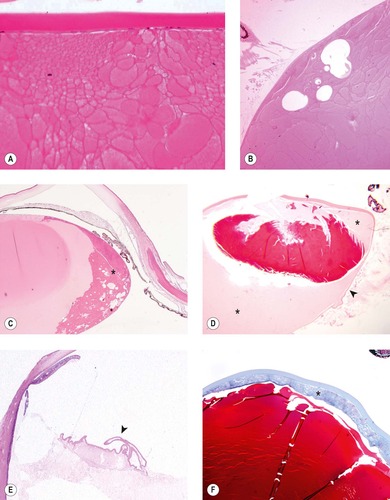
| Figure 10.1 The normal lens. (A) Gross photograph of normal canine lens in place in situ. (B) Photomicrograph of the anterior pole of a Davidson’s-fixed canine lens showing crisp outlines of individual lens fibers. (C) Photomicrograph of canine lens showing the equatorial lens nuclear bow. Cuboidal lens epithelial cells from the anterior pole first elongate, rotate and then become incorporated into the lens cortex (arrow). (D) Photomicrograph showing the posterior pole and posterior suture (*) of a canine lens in a Davidson’s-fixed specimen. (E) Gross photograph of a canine globe sectioned across the equator and postfixed in acetic acid to make the zonular ligaments more opaque. The photograph shows the distribution of zonular fibers. (F) Photomicrograph of the lens equator showing remnants of zonular ligament fibers (arrow). |
CONGENITAL OR HEREDITARY CONDITIONS (see Ch. 3)
Posterior lenticonus/lentiglobus (Fig. 10.2)
• Posterior lenticonus or lentiglobus is characterized by the localized axial elongation and increased curvature of the posterior lens, leading to a conical or spherical protrusion of the posterior pole of the lens
• Stretching, thinning or discontinuity of the posterior capsule are frequent findings in posterior lenticonus/lentiglobus.
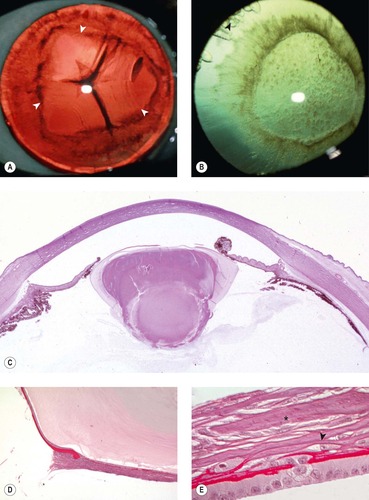 |
| Figure 10.2 Lenticonus. (A) Siberian Husky, 18 months old: the arrows delineate the area of posterior lenticonus. (B) Newfoundland, 1 year old: the dark irregular circle represents the area of lenticonus. Radiating cortical opacities and water vacuoles (arrow) are also present at the lens equator. (C) Low magnification photomicrograph of an equine eye showing posterior lenticonus. (D,E) Photomicrographs of the posterior pole from the same eye as (C) showing a complex relationship between the lens capsule and the proliferating lens epithelium. In (E), the lens epithelium has undergone spindle cell metaplasia (arrow) and collagen deposition (*). |
Aphakia, microphakia, lens coloboma (Fig. 10.3)
• Congenital absence of the lens, an abnormally small lens, or an irregular lens shape may result from developmental abnormalities affecting the orientation, induction and separation of the lens vesicle. Microphakia and irregularities of lens shape can be seen alone or, more often, as a part of a syndrome of developmental abnormalities involving the anterior segment of the globe
• Diffuse or focal lack of zonular tension at the lens equator may result in spherophakia or so-called lens coloboma respectively. These abnormalities in lens shape probably do not represent primary abnormalities in lens development, rather they are associated with anterior segment developmental abnormalities that affect the ciliary processes and zonular integrity.
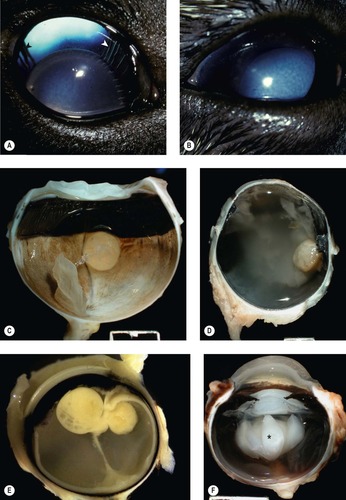 |
| Figure 10.3 Developmental problems of the lens. (A) Dachshund, 4 months old: in addition to being small, the lens was also rounder than normal (spherophakic). The ciliary processes with zonular fibers can be seen at both arrows. (B) German Shepherd Dog, 6 months old: the small round lens luxated totally into the anterior chamber, resulting in corneal edema. (C) Gross photograph of a canine globe with microphakia. (D) Photomicrograph of an equine globe with microphakia. (E) Bouin’s-fixed ferret globe with lens coloboma. (F) Gross photograph of canine globe with microphakia and posterior capsular rupture. Opaque lens proteins exude into the vitreous (*). |
Congenital cataract (Figs 10.4, 10.5)
• Morphologic features which typify congenital cataract include:
▪ Cataractous changes in the lens nucleus characterized by an abnormal position of the nucleus or lysis of the nucleus
▪ Abnormal relationship between the epithelium and lens capsule such as duplication, wrinkling, or segmental changes
▪ Posterior migration of lens epithelial cells
▪ Vascular or pigmented structures adherent to the lens capsule might indicate a cataract associated with abnormal development of the fetal vasculature (persistent pupillary membranes, persistent hyperplastic primary vitreous, or persistent hyperplastic tunica vasculosa lentis)
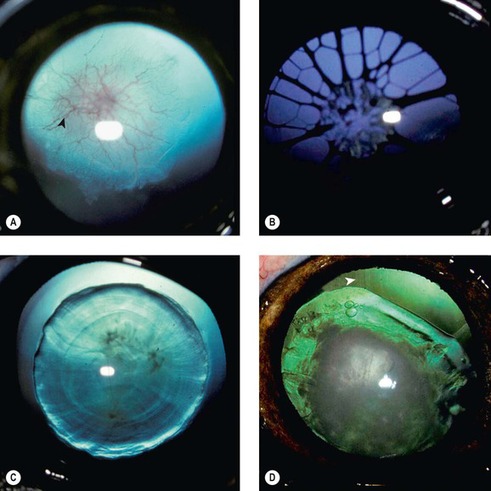 |
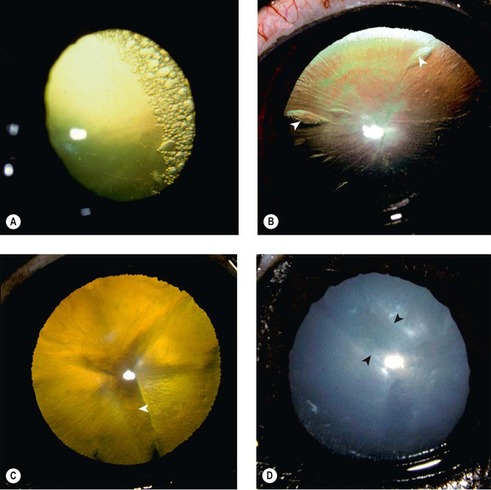
| Figure 10.4 Congenital and early onset cataract, clinical. (A) Labrador Retriever, 10 weeks old: posterior capsular and cortical opacity resulted from the persistent hyaloid artery and its branching vessels, persistent hyperplastic tunica vascularis lentis (arrow). (B) Great Dane, 8 weeks old: multiple persistent pupillary membranes attached to the axial anterior lens creating an anterior capsular opacity. (C) Boston Terrier, 3.5 months old: the diffuse nuclear opacity with clear cortex was present in both eyes. (D) Bassett Hound, 3 years old: the lens nucleus is totally opaque with diffuse cortical opacities. The lens has an irregular shape (coloboma). Fine zonular fibers are present only segmentally (arrow). |
 |
| Figure 10.5 Congenital cataract, pathology. (A) Low magnification photomicrograph of a dog lens with congenital cataract. The cataractous changes are predominantly nuclear. The posterior pole and the equatorial cortex remain near normal (arrow). (B) Low magnification photomicrograph showing a focal dysplastic and wrinkled lens capsule (arrow). (C) The same focus as (B) with higher magnification showing the relationship between the duplicated lens capsule and the lens epithelium. (D,E) Two photomicrographs of the anterior poles of two lenses showing duplications in the lens capsule and lens epithelium in canine congenital cataracts. |
• Congenital cataract and associated ocular abnormalities, that may include microphthalmia syndromes and abnormalities in the fetal hyaloid vasculature, are described in detail in Chapter 3.
Comparative Comments
• In man, as in animals, in addition to the congenital and hereditary abnormalities, primary aphakia with complete failure of lens formation has been reported in rare instances. More commonly, a small or incompletely formed lens, giving the clinical impression of aphakia, has been observed
• Other congenital abnormalities that are also seen the human lens include conditions of imperfect or delayed lens-corneal separation, anterior lenticonus, and spherophakia. In the latter condition, the lens is relatively more rounded than normal and usually smaller (microphakic)
• An important congenital condition in humans is rubella cataract, which occurs in the fetus if the mother is exposed to rubella virus during the first or second trimester of pregnancy. Rubella virus may be cultured from surgically removed lenses
• Although tumors of the lens do not occur in humans, the lens anlage has been reported to develop aberrantly in the lower lid, in a condition known as phakomatous choristoma.
CATARACT
• Cataract may be categorized according to extent of lens involvement, location within the lens, or etiopathogenesis.
Cataract categorized by the extent of disease (Figure 10.6, Figure 10.7, Figure 10.8, Figure 10.9 and Figure 10.10)
• Incipient cataracts involve less than 15% of the lens
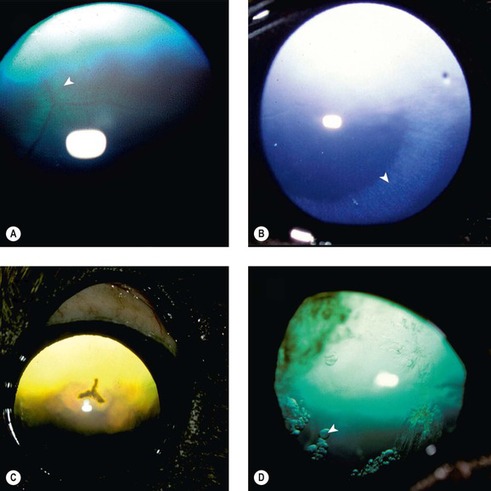 |
| Figure 10.6 Incipient cataracts, clinical. (A) Siberian Husky, 10 months old: feathering along the posterior cortical suture lines (arrow) was present in both lenses. (B) Cavalier King Charles Spaniel, 8 weeks old: the equatorial cortex was overhydrated (arrow) in this immature cataract. This overhydration cleared in the adult. (C) Golden Retriever, 3 years old: the posterior cortical suture is opaque as was the axial subcapsular cortex surrounding the suture line. (D) Italian Greyhound, 5 years old: equatorial cortical water vacuoles are present (arrow). The opacity at 10 o’clock represents vitreous degeneration. |
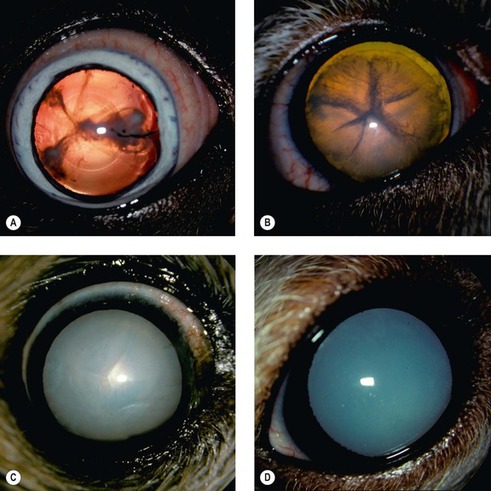 |
| Figure 10.7 Immature and mature cataracts, clinical. (A) Boston Terrier, 7 years old: anterior and posterior cortical opacities are present and radiate to the lens equator. (B) Cockapoo, 5 years old: the cortical suture lines are opaque. Diffuse cortical and nuclear opacities appear dark due to retroillumination from the tapetal reflection. (C) Pomeranian, 15 years old: the entire lens is opaque with no visible tapetal reflection in this mature cataract. (D) Poodle, 6 years old: the homogenous appearance of the cataract is due to lens liquefaction in this hypermature cataract. |
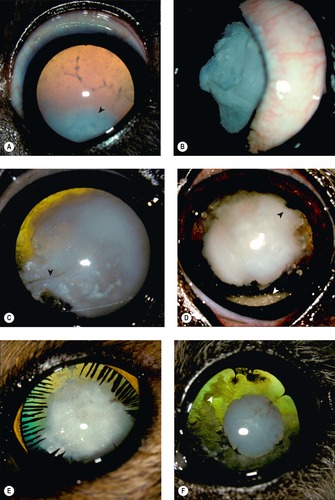 |
| Figure 10.8 Morgagnian cataract and lens resorption, clinical. (A) Poodle, 4 years old: the dense nucleus (arrow) has settled inferiorly in the fluid cortex in this Morgagnian cataract. (B) Cocker Spaniel, 6 years old: viewing the lens from the side showing the severely wrinkled anterior lens capsule. This was the result of chronic loss of lens protein. (C) Cocker Spaniel, 2 years old: the orange tapetal reflection can be seen following lens resorption. A linear wrinkle in the lens capsule is also visible (arrow). (D) Bichon Frise, 10 years old: the dense nucleus is present with several areas of posterior synechiae (black arrow). Liquefied cortical material is present within the inferior capsule (white arrow). (E) DSH, 5 years old: the lens has reduced significantly in diameter and is surrounded circumferentially by stretched ciliary processes adhered to the lens capsule. (F) Bichon Frise, 6.5 years old: the small opaque nucleus remains axially. Fragments of cortical lens material (arrow) are trapped between the anterior and posterior lens capsule. |
 |
| Figure 10.9 Classification of cataracts, pathology. (A) Photomicrograph showing cortical cataract, characterized by the presence of Morgagnian globules. (B) Bladder cells and Morgagnian globules in cortical cataract. A Morgagnian globule is a rounded lens fiber with no nucleus, and a bladder cell is a rounded fiber that contains a nucleus. (C) Photomicrograph of mature cataract showing extensive equatorial cortical pathology (*). (D) Hypermature Morgagnian cataract with wrinkling of the lens capsule (arrow) and remnants of lens nucleus floating in liquefied lens protein (*) within the capsule. (E) Low magnification photomicrograph showing the wrinkled lens capsule (arrow) after all the lens protein has been resorbed. (F) Hypermature cataract with extensive collagen-rich subcapsular cataract associated with spindle cell metaplasia of the lens epithelial cells (*). |
 |
| Figure 10.10 Diabetic cataract, clinical. (A) Keeshond, 9 years old: equatorial cortical water vacuoles were present circumferentially in both lenses. (B) Mixed Breed, 9 years old: equatorial water vacuoles were present. Fine radiations of cortical opacities and larger cortical water vacuoles (arrows) are present. (C) Rottweiler, 6 years old: this immature cataract has wide suture lines (arrow), which appear dark on retroillumination. Diffuse opacities throughout the overhydrated lens reduce the tapetal reflection. (D) Miniature Schnauzer, 9 years old: this intumescent lens is typical of the mature cataract seen in diabetes. The classical wide anterior cortical suture lines of an intumescent cataract are also observable (between arrows). |
• Immature cataracts affect more than 15% of the lens but lens involvement is incomplete and they do not completely obscure the fundus reflection
• Mature cataracts affect the lens cortex circumferentially and completely obstruct visualization of the fundus reflection
• Hypermature cataracts show evidence of lens shrinkage, such as lens capsule wrinkling, associated with leakage and resorption of altered cortical lens proteins.
Cortical cataract, the opacification of the lens fiber (Fig. 10.11)
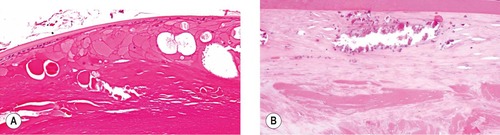 |
| Figure 10.11 Histopathologic indicators of cataract. (A) Photomicrograph showing a canine lens with Morgagnian globules and bladder cells, two reliable histologic indicators of cataract. (B) Photomicrograph of a canine lens with cortical mineralization. |
Subcapsular cataract, opacification and metaplasia of the lens epithelial cell (Fig. 10.12)
• Normal lens epithelial cells are positioned immediately adjacent to the lens capsule and their tropism for the lens capsule is seldom altered in disease states
• In subcapsular cataract the opacity is directly related to abnormalities of the lens epithelial cells
• Morphologic features of subcapsular cataract include:
▪ Proliferation of lens epithelial cells to form a localized aggregate
▪ Metaplasia, involving a change in the cells from an epithelial phenotype to a mesenchymal phenotype more characteristic of a myofibroblast
▪ Secretion of collagen around the metaplastic lens epithelial cells
▪ Loss of the lens epithelial cells leaving behind cell-free collagen matrix
▪ Mineralization.
 |
| Figure 10.12 Subcapsular cataract, pathology. (A) Photomicrograph showing lens epithelial hyperplasia and metaplasia in subcapsular cataract. (B) Photomicrograph showing a collagenous subcapsular cataract (*) (Alcian blue PAS). (C) Photomicrograph of a trichrome-stained lens with a collagenous subcapsular cataract. (D) Hypermature cataract with a wrinkled lens capsule and a contractile subcapsular cataract. |
Inherited cataract in dogs
• Inherited cataract is very common in the purebred canine population. An inherited basis for cataract development is proven or suspected in over 100 canine breeds, of which many appear to demonstrate complex patterns of inheritance. In some canine breeds, a genetic basis for cataract development has been clearly established, e.g. mutations in the HSF4 gene are associated with early-onset cataract in several breeds, including the Staffordshire bull terrier and Boston Terrier
• Clinical phenotype is highly variable between and within affected breeds. This variability may result from the influence of multiple genes and other metabolic and environmental factors.
Age-related cataract
• Cataracts are a common feature of senescence in most species
• Senile cataracts should be distinguished, both clinically and histomorphologically, from the normal process of nuclear sclerosis which is not associated with true lens opacity
• In nuclear sclerosis, the density of the lens nucleus increases with age as older lens fibers are progressively tightly packed centrally and take on a more homogeneous in appearance, as new cortical fibers are formed more peripherally.
Secondary cataract
• Metabolic cataract is recognized in almost all diabetic dogs (Fig. 10.10)
▪ Diabetic dogs are far more likely to develop cortical cataract because of the conversion of glucose to sorbitol within the lens cells and the resulting influx of water
▪ Diabetic cataracts often develop rapidly and can lead to serious inflammatory changes if the lens capsule ruptures (see below) or to secondary glaucoma caused by lens swelling (intumescent cataract)
▪ The diabetic state can also contribute to complications following cataract surgery
– In general, however, substantial differences in post-operative outcomes are not apparent compared to non-diabetic dogs
▪ Although diabetic cataracts are usually cortical cataracts, there are no specific morphologic features which allow a diabetic cataract to be distinguished from any other cortical cataract morphologically
▪ Although diabetes mellitus is fairly common in cats and humans, diabetic cataract is not common in these species
– The lower incidence of diabetic cataract in cats may relate to lower levels of activity of the enzyme aldose reductase in the lens of older cats, compared to dogs.
Comparative Comments
• The types of cataracts occurring in humans and other species appear to be extremely similar, although they have been further subdivided into a greater number of types in humans
• An extremely interesting entity is the exfoliation syndrome, also known as pseudoexfoliation, in which a fibrillary protein-like material is deposited on the anterior lens capsule
• The major systemic disorders associated with cataract development in humans are diabetes mellitus, galactosemia, hypercupremia, Fabry disease and Down syndrome
• Numerous drugs give rise to cataracts in humans, the most common being corticosteroids.
LENS PROTEIN BREAKDOWN OR LENS CAPSULE RUPTURE AND ITS SIGNIFICANCE IN INFLAMMATORY EYE DISEASE
Morphologic features suggesting pathologic lens capsule rupture (Fig. 10.13)
• Entrapment or digestion of lens capsule at the site of rupture is a feature of pathologic rupture
• If the lens capsule remains intact, then there should be no cell type other than lens epithelial cells or metaplastic lens epithelial cells within the capsule
▪ Characteristic cells to look for, that suggest pathologic lens capsule rupture, include the following:
– Macrophage cells
– Neutrophils
– Red blood cells
– Fibroblasts and blood vessels.
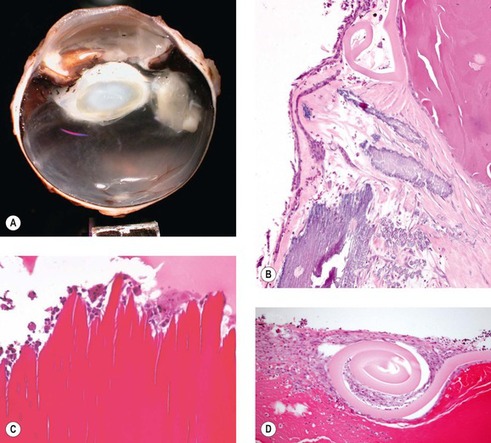 |
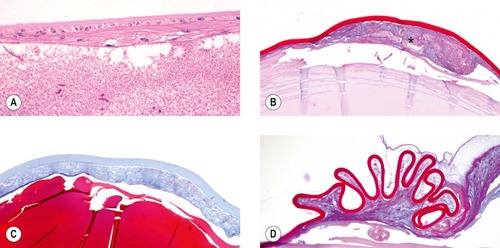
| Figure 10.13 Lens capsule rupture, pathology. (A) Gross photograph of a canine globe with lens capsule rupture, release of lens protein and phacoclastic uveitis. (B) Mineralization within subcapsular cataract exposed by lens capsule rupture which is characterized by a coiled lens capsule. (C) Photomicrograph showing the exposed lens fibers after lens capsule rupture and consumption of lens protein by phagocyte proliferation. (D) Lens capsule rupture with scrolling of the lens capsule and proliferation of lens epithelial cells. |
Phacolytic uveitis (lens-induced uveitis) (Fig. 10.14)
• Phacolytic uveitis occurs in response to the ‘broken down’ lens proteins that characterize cataract, particularly mature and hypermature cataract. These altered lens proteins are able to leak through an intact lens capsule into the aqueous inciting a mild to moderate inflammation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


