CHAPTER 127 Deep Digital Flexor Tendon Injuries in the Foot
Although it has long been suspected that injury to the digital portion of the deep digital flexor tendon (DDFT) is a potential cause of lameness originating in the foot, practitioners’ inability to use diagnostic imaging techniques to assess soft tissues inside the hoof has limited antemortem diagnosis of this condition. Consequently, previous reports consist of reviews of cases that were diagnosed postmortem. Since the advent of magnetic resonance imaging (MRI) and, to a lesser extent, computed tomography (CT), it has become clear that tendonitis of the DDFT is the most common soft tissue injury causing lameness in the equine foot. Tendonitis of the digital portion of the DDFT may occur alone, in conjunction with navicular bone pathology, or as one component of a complex of a multiple soft tissue injuries in the foot.
PATHOLOGY
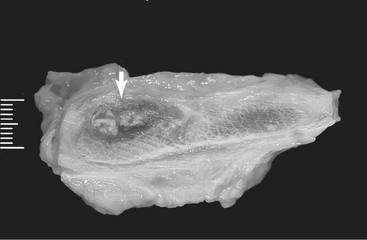
Recent pathologic surveys revealed four types of lesions in the digital portion of the DDFT: core lesions, sagittal plane splits, insertional lesions (enthesopathy), and dorsal border lesions. Core lesions (Figure 127-1) are characterized by gross fiber disruption in the center of usually only one lobe. Core lesions most frequently span the upper extent of the T-ligament into the proximal recess of the navicular bursa but can extend a variable distance proximodistally and occasionally cause a continuous core defect from the insertion to the level of the distal aspect of the proximal phalanx.
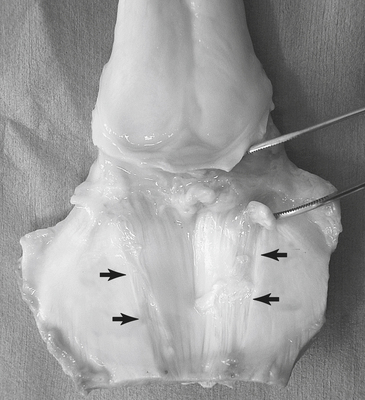
Sagittal plane splits (Figure 127-2) develop mostly in the navicular bursal portion of the DDFT, at the level of the flexor surface of the navicular bone, and can extend proximodistally. The depth of a sagittal plane split may vary from superficial, extending no more than 20% through the thickness the affected lobe, to deep, extending from the dorsal surface to the palmar surface of the DDFT.

Insertional lesions (Figure 127-3) are limited to the distal 10 to 20 mm of the DDFT near its insertion on the distal phalanx. They consist of small core lesions, sagittal plane splits, or osseous changes at the insertion site. Core lesions and sagittal plane splits can be encountered in this location as a distal continuation of more proximal lesions or may occur in isolation. Osseous changes of enthesopathy include focal cortical bone loss, cyst formation, entheseous new bone production, and sclerosis.

Lesions of the dorsal border of the DDFT (Figure 127-4) are found primarily in the navicular bursa and consist of superficial fibrillations or diffuse lesions communicating with the dorsal margin of the DDFT. Dorsal DDFT erosions and abrasions consist of longitudinal strips of superficial fiber damage extending the length of the navicular bursa. Although other DDFT lesions frequently develop without abnormalities of the navicular bone, lesions of the dorsal border are invariably accompanied by degenerative changes of the palmar surface of the navicular bone. Not infrequently, fibrillated tendon fibers adhere to exposed areas of the flexor cortex.
CLINICAL EXAMINATION
Visual Inspection and Palpation
There are generally no visual or palpable abnormalities that indicate injury of the digital portion of the DDFT as the cause of lameness. Occasionally distension of the digital synovial sheath is seen in horses with a lesion that extends proximally to the level of the sheath. Even more rarely a focal, painful, firm soft tissue swelling can be appreciated on the palmar aspect of the DDFT in the distal aspect of the pastern.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


