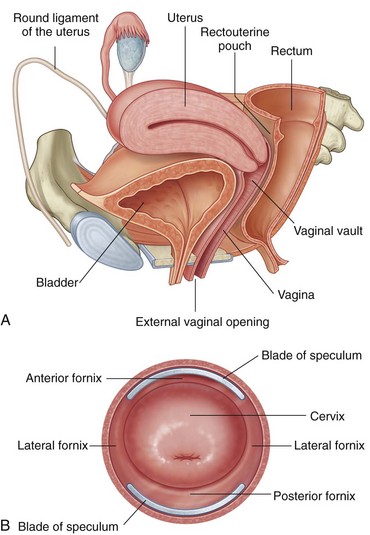
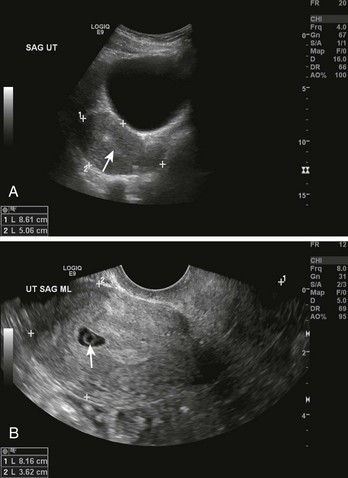
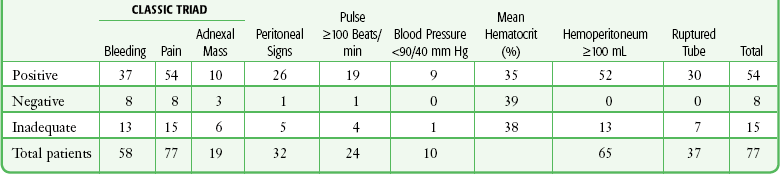
Chapter 57 Culdocentesis is a procedure in which a hollow needle is inserted through the posterior vaginal wall into the peritoneal space to obtain peritoneal fluid for analysis and culture. This procedure is simple, rapid, and safe. The technique is used primarily to diagnose ruptured ectopic pregnancies and ruptured ovarian cysts and, rarely, to obtain material for culture to aid in the diagnosis of pelvic inflammatory disease (PID). The availability of bedside ultrasound, high-resolution transvaginal ultrasound, and highly sensitive β-human chorionic gonadotropin (β-hCG) assays has led to a decline in the use of this procedure. Despite this change, culdocentesis is still valuable in patients in whom a ruptured ectopic pregnancy is suspected but who are too unstable to transport for a formal sonographic examination.1 Before attempting culdocentesis, the clinician must be familiar with the anatomy of the vagina and the rectouterine pouch (pouch of Douglas) (Fig. 57-1). In adult women, the vagina is approximately 9 cm long. From its inferior to its superior aspect, the posterior wall of the vagina is related to the anal canal by way of the perineal body, the rectum, and the peritoneum of the rectouterine pouch.2 The uterus lies at nearly a right angle to the vagina. The rectouterine pouch and the posterior wall of the vagina are adjacent only at the upper quarter (≈2 cm) of the posterior vaginal wall. The vaginal wall in this area is less than 5 mm thick. Culdocentesis is indicated in any adult woman in whom aspiration of fluid from the rectouterine pouch will help confirm the clinical diagnosis. If ultrasound examination is not readily available in the emergency department (ED) or if the patient is too hemodynamically unstable to be transported to an off-site location for ultrasound, culdocentesis may be the fastest and most accurate diagnostic technique available to the emergency clinician.3 Analysis of peritoneal fluid is also a reliable method of differentiating inflammatory from hemorrhagic pelvic pathologic conditions. Conditions in which culdocentesis may be of diagnostic value include a ruptured viscus (particularly an ectopic pregnancy or a corpus luteum cyst), PID and other intraabdominal infections (particularly appendicitis with rupture or diverticulitis with perforation), intraabdominal injuries to the liver or spleen, and ruptured aortic aneurysms.4 Ectopic pregnancy is often one of the most difficult gynecologic lesions to diagnose.5 The incidence of ectopic pregnancy is on the rise, and it accounts for 1.6% of all pregnancies. Ectopic pregnancy is the most common obstetric cause of maternal death in the first trimester.5 In a series of 300 consecutive cases of ectopic pregnancy, 50% of patients received medical evaluation at least twice before the correct diagnosis was made.6 In 11% of patients in this series, the diagnosis was not made until the third medical visit. The clinical picture of ectopic pregnancy may include vascular collapse, pelvic pain, isolated rectal or back pain, amenorrhea, abnormal menses, shoulder pain, syncope, cervical or adnexal tenderness, adnexal mass, anemia, and leukocytosis. It is important to note that blood in the peritoneal cavity does not consistently correlate with peritoneal irritation, blood pressure, or pulse rate.7 In fact, bradycardia in the presence of significant intraperitoneal bleeding from a ruptured ectopic pregnancy is not unusual (Tables 57-1 and 57-2). TABLE 57-1 From Cartwright PS, Vaughn B, Tuttle D. Culdocentesis and ectopic pregnancy. J Reprod Med. 1984;29:88. TABLE 57-2 From Cartwright PS, Vaughn B, Tuttle D. Culdocentesis and ectopic pregnancy. J Reprod Med. 1984;29:88. Risk factors for an ectopic pregnancy include a history of salpingitis, use of an intrauterine contraceptive device, or tubal ligation; however, no combination of these signs, symptoms, or historical data is diagnostic of an ectopic pregnancy. To confuse the diagnosis further, a normal menstrual history is reported in approximately 50% of patients with an ectopic pregnancy. A urine pregnancy test is occasionally negative.8 Though rarely seen, the combination of a uterine decidual cast (Fig. 57-2) and a positive pregnancy test is virtually pathognomonic of an ectopic pregnancy. A uterine cast is decidua that has been hormonally stimulated by the ectopic pregnancy but is passed vaginally when the tissue can no longer be supported. The cast is an outline of the uterine cavity, but it can be mistaken for products of conception if not inspected carefully. Therefore, all tissue passed vaginally should be carefully inspected before being sent to the laboratory for analysis for products of conception. An ectopic pregnancy can occasionally occur in conjunction with an intrauterine pregnancy. Patients who have undergone a therapeutic abortion may actually have had an unrecognized ectopic pregnancy, hence the need for pathologic evaluation of any tissue obtained by uterine evacuation procedures. The greater sensitivity of the serum and urine β-hCG assay, coupled with the increased availability of emergency medicine physicians trained to perform pelvic ultrasound, has greatly increased the chance of early diagnosis of unruptured and ruptured ectopic pregnancy.9 Urinary β-hCG tests provide a sensitivity to 20 to 50 mIU/mL and are positive in the first few weeks of pregnancy. However, ectopic pregnancy is often associated with very low production of this hormone. Quantification of the serum test adds additional information since it is sensitive to 5 mIU/mL. Therefore, a negative urine β-hCG test rules out pregnancy in greater than 98% of cases, and pregnancy in any site can be ruled out in virtually all patients with a negative serum β-hCG test.10 A single quantitative β-hCG level is a poor predictor of the size of the pregnancy or the risk for ectopic pregnancy, but serial testing is quite helpful. It is expected that the quantitative serum β-hCG level should double approximately every 2 days in the first trimester. To increase the accuracy of diagnosis, it is helpful to combine quantitative β-hCG testing with ultrasound examination (Fig. 57-3). An empty uterus by transvaginal or abdominal ultrasound combined with certain quantitative serum β-hCG results can be quite helpful to the clinician. The quantitative range in which the ultrasonographer should detect an intrauterine pregnancy varies, but an intrauterine pregnancy should be detected if the serum β-hCG level is in the range of 1200 to 1500 mIU/mL when using a transvaginal probe and greater than 6000 mIU/mL when using a transabdominal probe. Endovaginal ultrasonic scanning consistently identifies a 4-week gestational sac if the β-hCG level is 2000 mIU/mL or greater. The presence of a fetal pole and cardiac activity are detectable with endovaginal ultrasound scanning at approximately 6 and 7 weeks, respectively.11 Note that a heartbeat can occasionally be detected in an ectopic pregnancy or in an extrauterine pregnancy and may be mistakenly deemed intrauterine. It is important to note that the absence of an intrauterine pregnancy by ultrasound, when the β-hCG level is below the discriminatory zone (defined as the hCG level at which a normal intrauterine pregnancy can be detected by ultrasound), is nondiagnostic and could represent an early viable normal pregnancy, a nonviable intrauterine pregnancy, a completed abortion, or an ectopic pregnancy. When no intrauterine pregnancy is detected by ultrasound and the serum β-hCG level exceeds the discriminatory zone, the chance of an ectopic pregnancy ranges from 86% to 100%.12
Culdocentesis
Anatomy
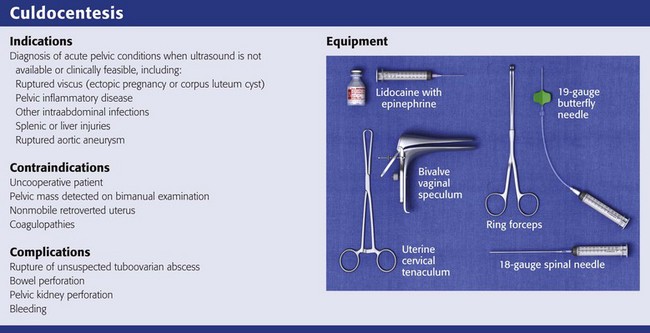
Indications
Ectopic Pregnancy

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Culdocentesis