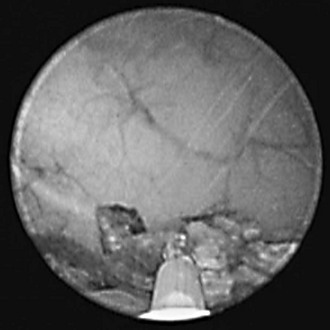
Web Chapter 70 Mineral composition of uroliths and their size, number, and location are important considerations in the selection of minimally invasive procedures (e.g., voiding urohydropropulsion, laparoscopic-assisted cystotomy, and laser lithotripsy) for urolith management in dogs and cats (see Chapter 203 in the previous edition of Current Veterinary Therapy). Voiding urohydropropulsion may be used to remove uroliths that are smaller than the diameter of the dilated urethra (typically less than 3 to 4 mm in diameter). Laser lithotripsy effectively extends the use of voiding urohydropropulsion to larger uroliths by fragmenting uroliths into smaller pieces before transurethral evacuation (Web Figures 70-1 and 70-2). However, laser lithotripsy is not suited ideally to every patient. In small male dogs (≤5 kg) and all male cats, the lumen of the urethra may not dilate sufficiently to accommodate insertion of cystoscopies to permit urolith management. Web Figure 70-1 Cystoscopic view of laser lithotripsy of a calcium oxalate urolith within the bladder lumen of a female dog. The quartz laser fiber tip is in direct contact with the urolith surface. Small urolith debris can be seen as streaks within the saline used to distend the urinary bladder. Web Figure 70-2 Multiple urolith fragments in bladder lumen after laser lithotripsy fragmentation of the calcium oxalate urolith. The remaining urolith fragments are small enough to pass through the urethra. Laser lithotripsy is performed with urolith visualization by urethrocystoscopy. Detailed description of urethrocystoscopy is beyond the scope of this chapter and has been described elsewhere (Adams, 2006). The authors prefer to position female dogs and cats in dorsal recumbency and male dogs in lateral recumbency for laser lithotripsy. The area around the vulva or prepuce is clipped to remove surrounding hair and prepped for aseptic introduction of the cystoscope into the urethra and bladder. During cystoscopy irrigation of sterile warmed normal saline or sterile water is used to distend the urinary tract and facilitate cystoscope passage. Once the uroliths are visualized in the urethra or bladder, a flexible quartz laser fiber is advanced through the working channel of the scope and connected to the laser unit. During laser activation the energy is limited to an area directly in front of the quartz laser fiber tip. An aiming beam within the visible spectrum is used to facilitate targeting the laser energy. The laser fiber should not be aimed directly at the mucosal surface and should be kept 0.5 mm or more away from the mucosal surface during laser activation. Therefore it is preferable to apply laser energy to the urolith surface while working parallel rather than perpendicular to the mucosa (see Web Figures 70-1 and 70-2). In the event of brief laser application directly to the mucosal surface, mucosal injury usually is limited to superficial damage and minimal bleeding. When in contact with the mucosal surface, the Ho:YAG laser is capable of making incisions into the bladder or urethral wall; perforation is possible during laser lithotripsy. The Ho:YAG laser can be used effectively in contact mode to remove small pedunculated polyps or tumors within the urinary tract without creating full-thickness incisions. With proper technique the risk of bladder or urethral perforation is minimal during laser lithotripsy.
Laser Lithotripsy for Uroliths

Laser Lithotripsy Technique
Chapter 70: Laser Lithotripsy for Uroliths
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


