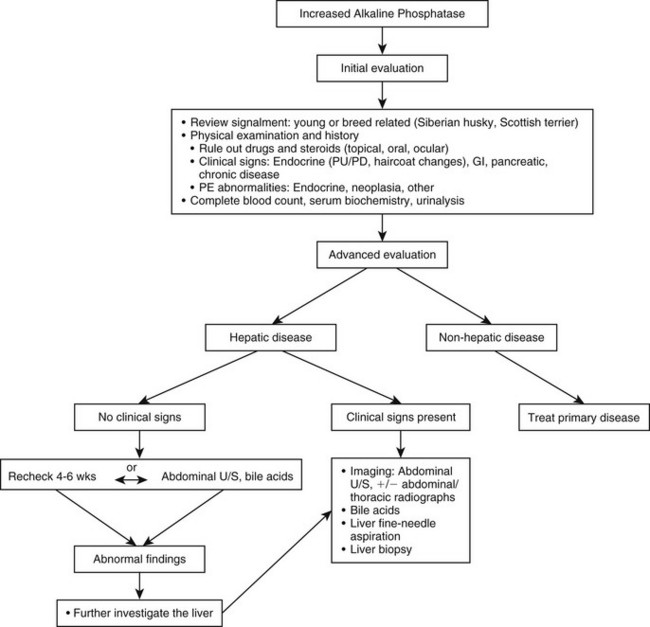
Web Chapter 50 Increased serum alkaline phosphatase (ALP) is a common laboratory finding in canine patients. In one survey of consecutive blood samples submitted to a reference laboratory, 39% of all dogs and 51% of dogs older than 8 years of age had increased ALP levels (Comazzi et al, 2004). The high sensitivity (86%) of increased ALP for detection of liver disease is complicated by the poor specificity (49%) because numerous diseases outside of the liver, as well as drugs and glucocorticoids, may induce production of the enzyme. Often the evaluation of canine patients with increased ALP becomes a diagnostic dilemma. L-ALP induction also occurs secondary to various drugs, most notably phenobarbital and endogenous or exogenous glucocorticoids. The underlying pathophysiologic mechanisms are poorly understood. Elevated L-ALP, B-ALP, and C-ALP were found in one study after phenobarbital administration, a finding most consistent with induction because all isoenzymes were affected (Gaskill et al, 2004). However, differences in total L-ALP were not found between treated and untreated dogs in a separate study, an unexpected finding if induction was the primary mechanism (Gaskill et al, 2005). Increased serum levels may be secondary to increased activity of GPI phospholipase and subsequent release of ALP in serum or by direct liver injury, causing cholestasis. Glucocorticoids have been shown to increase serum C-ALP and L-ALP through induction by increasing levels of messenger ribonucleic acid (mRNA) within 24 to 48 hours of exposure. C-ALP is a product of the I-ALP gene that differs from I-ALP only in carbohydrate composition. I-ALP is devoid of carbohydrates, whereas C-ALP is glycosylated heavily with sialic acid and is thought to be responsible for the different half-lives of the two enzymes. The hepatocyte is the site of de novo synthesis of C-ALP after exposure to endogenous and exogenous glucocorticoids (Wiedmeyer et al, 2002). Expression of the I-ALP gene in the liver is delayed after exposure to steroids, as shown by increased mRNA expression and elevated L-ALP and serum C-ALP approximately 10 days after initiation of prednisone in experimental dogs. C-ALP accumulates on hepatocyte membranes in the area that composes the bile canaliculi and sinusoidal surfaces, and elevated serum levels occur through solubilization of C-ALP by activity of GPI phospholipase. Total ALP can be quantified further by determining the percent of C-ALP isoenzyme in the serum using electrophoresis, selective inhibition (levamisole treatment), or a heat inactivation process in the laboratory. Measuring the isoenzymes of ALP is an available assessment in most diagnostic laboratories but often is of little clinical use. For example, the high sensitivity (95%) of elevated C-ALP for detection of hyperadrenocorticism (HAC) is complicated by the poor specificity (18%). Elevations in C-ALP are often present with diabetes mellitus (DM), primary liver disease, or other chronic illness possibly because of stress and increases in endogenous cortisol. Although finding increased C-ALP cannot confirm the presence of HAC, it generally is accepted that low values of C-ALP decrease the likelihood of this disease. Progesterones also are thought to bind to the corticosteroid receptor on the hepatocyte and may induce C-ALP production; however, this has been more recently questioned (see Chapters 50 and 148). Phenobarbital has also been shown to induce production of the C-ALP isoenzyme through unknown mechanisms. Evaluation of the patient with elevated ALP begins with a thorough history and physical examination (Web Figure 50-1). The signalment may provide insight as to the underlying cause of ALP elevation. For instance, mild elevations in ALP (<2× normal) often are present in young, growing animals because of increased B-ALP. Often the calcium and phosphorous also are increased mildly in these dogs, and all three are expected findings in young dogs. Postsuckling puppies also have increases in ALP, possibly as a result of colostral ALP or induction of ALP after ingestion of colostrum. Values typically return to normal within 10 days. Because elevated ALP may occur as a result of enzyme induction, a careful drug history should be obtained. Commonly identified drugs include glucocorticoids and phenobarbital. In addition to oral steroids, topical and ocular forms also may be associated with increased ALP. Specific questioning usually is needed to ensure that other forms of steroids are not being given because topical therapy often is not considered a medication by owners and frequently is not disclosed without direct questioning. Exposure to phenobarbital or other anticonvulsants often is determined easily, but other drugs also have been associated with elevated liver enzymes and liver toxicity and are discussed elsewhere (see Chapter 140). Various holistic herbal and nutritional supplements also may induce the production of ALP or cause liver damage. Discontinuation of the substance and subsequent resolution of ALP elevation over the following weeks is consistent with drug-induced abnormalities. When an elevation in serum ALP is identified, routine blood work, including complete blood count, a comprehensive serum biochemistry, and urinalysis, should be performed. Primary hepatic disease, secondary reactive hepatopathies, and induction caused by drugs are the most likely causes. Common causes are listed in Web Box 50-1. Nonhepatic disease is a common cause of ALP elevations, resulting from secondary reactive changes (reactive hepatopathies) occurring in the liver. Potential causes include enteritis, pancreatitis, or systemic inflammatory or infectious diseases. Histologic evidence of disease as indicated by a variety of nonspecific reactive changes (e.g., hydropic change and periportal inflammation) often is present. Typically ALP values are threefold to fourfold above normal. Elevations in C-ALP also can result from chronic illness and endogenous glucocorticoid release. Both conditions generally cause only mild ALP elevations.
Evaluation of Elevated Serum Alkaline Phosphatase in Dogs
Pathophysiology
Liver Alkaline Phosphatase
Corticosteroid Alkaline Phosphatase
Diagnostic Evaluation
History and Physical Examination
Preliminary Evaluation