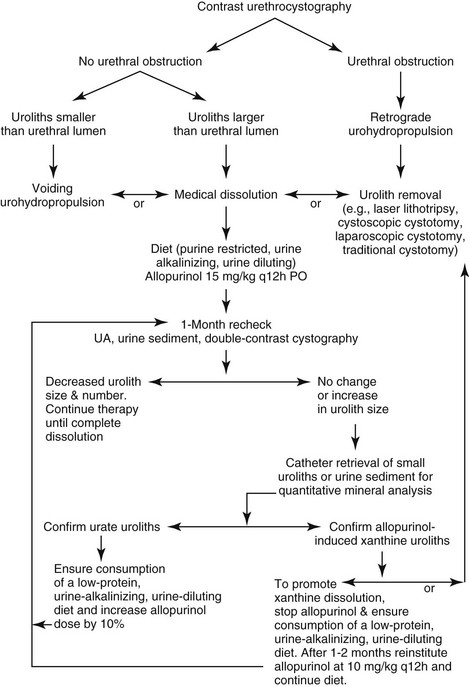
Chapter 198 Risk factors associated with urate lithogenesis in dogs include the following: 1. Increased renal excretion and urine concentration of uric acid 2. Increased renal excretion or renal production of ammonium ions 3. Increased microbial production of ammonium ions 5. Formation of highly concentrated urine 6. Presence of promoters or absence of inhibitors of urate urolith formation Genetic factors also may be important. Hyperuricuria and urate urolithiasis have been linked to a mutation in a urate transporter that was identified recently in dalmatians, English bulldogs, and Black Russian terriers and sporadically in other breeds (Karmi et al, 2010). Efficacy of medical dissolution depends on several key factors: the location of the uroliths, the treatments selected, owner compliance with the treatment regimen, any underlying disease(s), and disease severity. In an uncontrolled clinical trial, 25 dogs with naturally occurring urate urocystoliths (without hepatic portovascular anomalies) were prescribed canned Hill’s Prescription Diet u/d and allopurinol (15 mg/kg q12h). Of these dogs, 36% experienced complete dissolution (median dissolution time, 3.5 months), 32% experienced partial dissolution, and 32% experienced no dissolution (Osborne et al, 2009). Aside from sporadic anecdotal reports, we are not aware of the efficacy of other potentially litholytic diets (e.g., vegetarian diets, Royal Canin Veterinary Diet Urinary UC Low Purine, and other lower-protein diets formulated for dogs with renal failure, liver disease, or dermatologic disorders). The role of a new selective xanthine oxidase inhibitor, febuxostat (Uloric), in safely promoting effective urolith dissolution also is unknown. Unlike allopurinol, febuxostat does not need to undergo hepatic transformation to more active metabolites. Therefore febuxostat would appear more suitable for dogs with portovascular shunts and urate urolithiasis; however, abnormal liver function test results were a frequent adverse event in humans taking the medication. Additional clinical studies are needed to evaluate the efficacy of contemporary diets and newer medications. Until such studies are completed, we recommend initially considering evidence-based medical dissolution therapies for dogs with asymptomatic or mildly symptomatic urate urocystoliths and nephroliths (Figure 198-1). More rapid urolith removal (surgery, lithotripsy, cystoscopically assisted cystotomy, or laparoscopic cystotomy) should be considered for dogs with urethroliths and clinically active disease (e.g., moderate to severe clinical signs or urinary obstruction). 2. Place 10 ml of the remaining mixture in a 10- to 15-ml cone-tipped centrifuge tube. Centrifuge the sample to separate the sediment from the solution (alternatively, the sample can sit undisturbed to allow for separation by gravity). 3. Decant the supernatant again. 4. Repeat this process by adding additional urine to the centrifuge tube until sufficient sediment (i.e., 0.5- to 1-cm depth) is reclaimed. 5. Allow the sediment to air-dry for several days before submitting it for quantitative mineral analysis.
Canine Urate Urolithiasis
How Effective Is Medical Dissolution of Urate Uroliths?
How Should Medical Dissolution Be Monitored?
Large Urine Sample
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Canine Urate Urolithiasis
Only gold members can continue reading. Log In or Register to continue
