4 Blepharitis
CLINICAL EXAMINATION
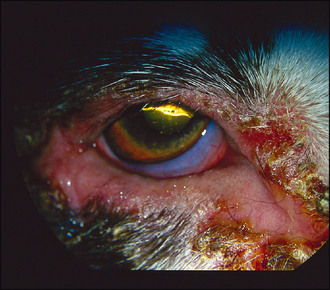
Ophthalmic examination will reveal eyelid swelling and hyperaemia, possibly with crusting or exudative erosions close to the eyelid margins (Figure 4.1). Some lesions are erosive and a serosanguinous discharge can be present (Figure 4.2). Periorbital hyperaemia or alopecia could be signs of self-trauma. Close examination of the eyelids themselves might reveal multiple swellings along the lid margin in the location of the meibomian glands – suggestive of a meibomianitis (Figure 4.3). Schirmer tear test readings should be checked in all cases.


CASE WORK-UP
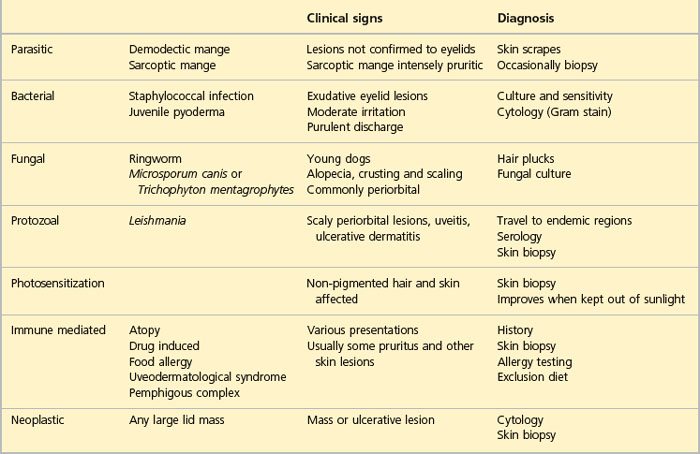
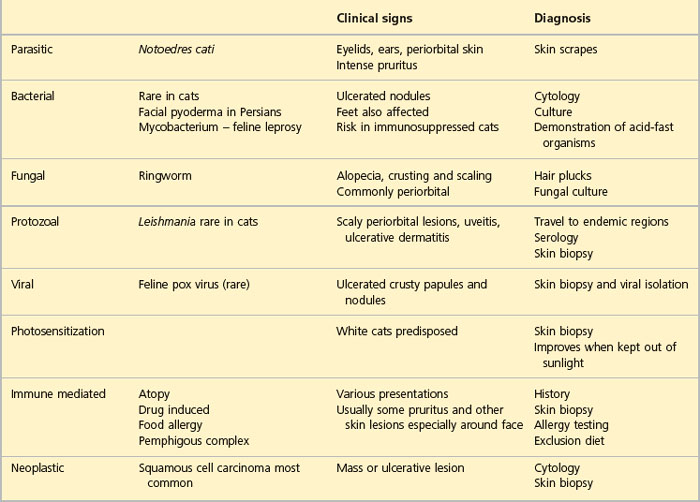
Once a thorough general clinical and ophthalmic examination has been performed the appropriate diagnostic tests can be initiated. In many cases swabs for bacterial culture and sensitivity should be taken – both from the ocular discharge and from exudations from the lid margins themselves. Samples for parasitic isolation should also be considered so several swabs might be required in different transport media. Impression smears of the lid margins can be useful, and scrapes and hair plucks to look for parasites can be rewarding. If Leishmania is suspected then serological testing is advised. Additionally, many cases benefit from biopsy – especially since the commonly found bacterial infection might not be the underlying problem – with allergic reactions and immune-mediated disease high on the list of potential underlying conditions. Biopsy specimens should include the eyelid margin whenever possible – a small wedge resection is removed under general anaesthesia and sutured with 6/0–4/0 soft material (such as polyglactin 910, although care should be exercised using braided suture in the face of infection). If meibomian gland involvement is present, samples of inspissated matter can be curetted from the swellings and sent for both bacterial culture and cytology. Biopsy samples from other skin lesions should be considered. If atopy is suspected, then intradermal skin tests can be performed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


