Heather K. Knych
Analgesic Pharmacology
Perception of pain begins with stimulation of nociceptors located in tissues. Stimulation of these nociceptors, whether from chemical or physical (heat, cold, or mechanical pressure) signals generates an impulse that travels to the dorsal horn, where it stimulates second-order neurons in the spinal cord gray matter. Signals are transmitted to the second-order neurons through fast-conducting (A delta) or slow-conducting (C) fibers. Finally, the signal is transmitted through specific pathways to the thalamus, brainstem, and limbic system. Chemical mediators, released in response to stimulation of the pain pathways, function in transmission of peripheral pain as well as signal processing in the dorsal horn. Glucocorticoids, endogenous opioids, catecholamines, endorphins and enkephalins, substance P, excitatory and inhibitory neurotransmitters (aspartate, γ-aminobutyric acid, and prostaglandins), and monoamines appear to be the most prominent. These mediators serve as important targets for pharmacologic intervention (Table 13-1).
TABLE 13-1
Analgesics Commonly Used in Horses in the United States
| Drug | Formulation | Route | Dose (mg/kg) | |
| NSAIDs | ||||
| Phenylbutazone | Tablets, paste, Powder Injectable | PO IV | 4.4 mg/kg q 24 hr 2.2 mg/kg q 12 hr 2.2-4.4 mg/kg q 12 hr | |
| Flunixin | Injectable Paste, granules | IV, IM PO | 1.1 mg/kg q 24 hr 1.1 mg/kg q 24 hr | |
| Ketoprofen | Injectable | IV | 2.2 mg/kg q 24 hr | |
| Firocoxib | Injectable Paste | IV PO | 0.09 mg/kg q 24 hr 0.1 mg/kg q 24 hr | |
| Diclofenac | Liposome-cream | Topical | 73 mg (5-inch strip) q 12 hr | |
| α2-Receptor Agonists | ||||
| Xylazine | Injectable | IV IM | 0.2-1.1 mg/kg 0.6-2.2 mg/kg | |
| Detomidine | Injectable | IV IM | 0.02-0.04 mg/kg 0.02-0.04 mg/kg | |
| Romifidine | Injectable | IV | 0.04-0.12 mg/kg | |
| Opioids | ||||
| Butorphanol | Injectable | IV | 0.01-0.1 mg/kg | |
| Morphine | Injectable | IV | 0.2-0.6 mg/kg* | |
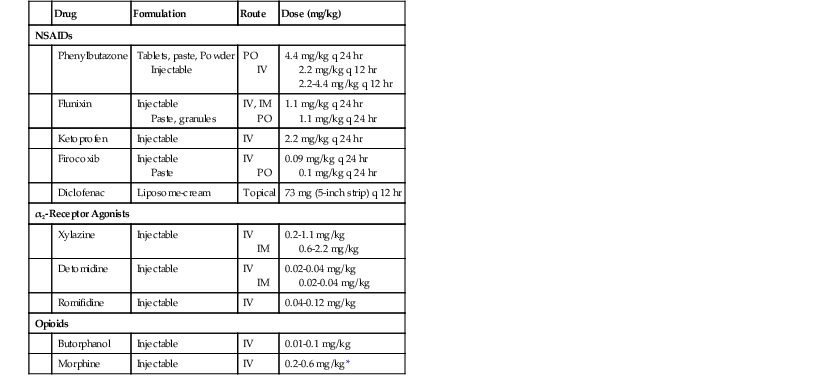
* Administer in combination with acepromazine (0.05 mg/kg IV), xylazine (0.5-1.0 mg/kg IV), or detomidine (0.01-0.02 mg/kg IV) to reduce excitement.
Nonsteroidal Antiinflammatory Drugs
Nonsteroidal antiinflammatory drugs (NSAIDs) are arguably the most commonly used class of drugs for managing pain in horses. Although these drugs are classified as antiinflammatory drugs, they are also analgesics by virtue of their antiinflammatory effects. Tissue damage results in the release of inflammatory mediators, including prostaglandins. The primary mechanism of action of NSAIDs is inhibition of cyclooxygenase (COX) enzymes, which are involved in the production of prostaglandins. To date, three COX enzymes (COX-1, COX-2, and COX-3) have been identified. COX-1, which is constitutively expressed, is often referred to as the “housekeeping” COX enzyme. It plays a role in blood clotting, regulation of vascular homeostasis, renoprotection, gastroprotection, and coordination of the actions of circulating hormones. Many of the adverse effects associated with chronic administration of NSAIDs in the horse have been attributed to inhibition of COX-1 and include gastrointestinal irritation and ulceration, renotoxicity, hepatotoxicity, inhibition of hemostatic mechanisms, blood dyscrasias, and delayed parturition, soft tissue, and fracture healing. However, although in some cases adverse effects associated with COX-1 inhibition can be severe, in most horses, these side effects are minimal at therapeutic doses. Nonetheless, in an attempt to decrease the side effects observed with nonselective NSAID administration, NSAIDs capable of selectively inhibiting COX-2 have been developed. The COX-2 enzyme is both constitutive (always expressed) and inducible, depending on the organ system involved. Although COX-2 is generally associated with the harmful effects of the inflammatory process, in actuality it generates both proinflammatory and antiinflammatory cytokines and can play a protective role (e.g., in renal homeostasis). The inducible and potentially damaging form of COX-2 is stimulated by proinflammatory cytokines, growth factors, lipopolysaccharide, and mitogens.
Phenylbutazone, flunixin, and ketoprofen remain the most commonly used NSAIDs in equine medicine. All are classified as nonspecific COX inhibitors because they inhibit both COX-1 and COX-2 enzymes. Although side effects associated with inhibition of COX-1 enzymes have been reported, when used at recommended doses and for a short duration, adverse effects are rare. Phenylbutazone, flunixin, and ketoprofen are all labeled for alleviation of pain and inflammation associated with the musculoskeletal system, and flunixin is also used for treatment of visceral pain associated with colic. The onset of effect is within 2 hours for both flunixin and ketoprofen, with peak effects observed within 12 to 16 hours for both. Most NSAIDs have relatively short plasma elimination half-lives (1 to 6 hours); however, effects following a single administration have been reported to last up to 24 hours for phenylbutazone and 30 hours for flunixin.
Firocoxib1 is a COX-2 selective NSAID that is being used with increasing frequency in equine medicine because of its purported favorable safety margin compared with nonselective NSAIDs. Firocoxib is used to manage musculoskeletal pain and lameness associated with osteoarthritis in horses. In 2012, Orsini and colleagues found that improvement in lameness scores was observed within the first 7 days after starting treatment. Relative to other NSAIDs used in equine medicine, firocoxib bioaccumulates after chronic administration, has a prolonged elimination half-life (36.5 hours following oral administration), and can be detected for up to 26 days after administration of the final dose of a 14-day treatment regimen. Another firocoxib formulation2 has been approved for use in dogs. Anecdotally, it appears to be effective when administered to horses, but there are no published studies describing the absolute or relative bioavailability of this product in horses.
Diclofenac is another NSAID used in horses. It is available in a liposome-based cream for topical administration.3 The reported benefit of this formulation is that it provides a local antiinflammatory effect with minimal systemic absorption, which reportedly reduces the side effects noted with other nonselective NSAIDs.



