Chapter 10 Ambulatory electrocardiography and heart rate variability
ELECTRODE PLACEMENT FOR AMBULATORY ELECTROCARDIOGRAPHY
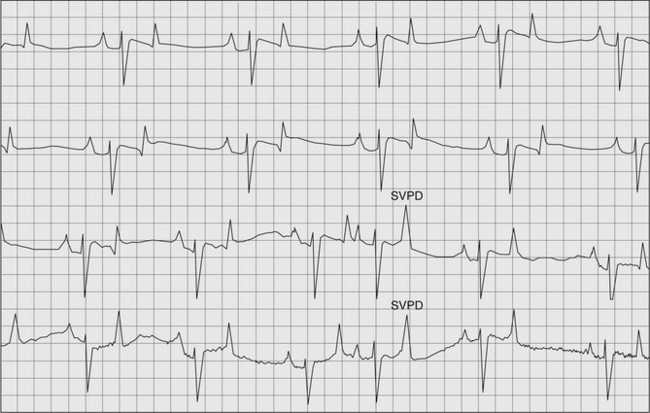
In order to obtain a diagnostic ambulatory ECG it is usual to use a chest-lead system so that electrodes can be placed underneath a girth or surcingle that will ensure appropriate contact between the electrode and the skin, will reduce movement artifact and will provide a point for attachment of the device. In order to optimize the ECG for automated processing the lead placement is usually such that the positive electrode (right arm) is placed at the top of the thorax on the left-hand side at the level of the vertebral bodies while the negative electrode (left arm) is placed on the sternum. If multiple leads are being used the neutral (left leg) is placed on the right-hand side of the thoracic wall. The earth (right leg) electrode can be placed anywhere around the girth area. It is usual to clip the horse where the electrodes will be placed and to use self-sticking electrodes that contain contact gel. It may be necessary to apply surgical spirit to maintain electrical contact especially in hot climates. The girth should be applied tightly to prevent movement of the electrodes. This arrangement of electrodes should record an ECG with a negative QRS, positive P and T waves (Fig. 10.1).
RESTING AMBULATORY ELECTROCARDIOGRAPHY
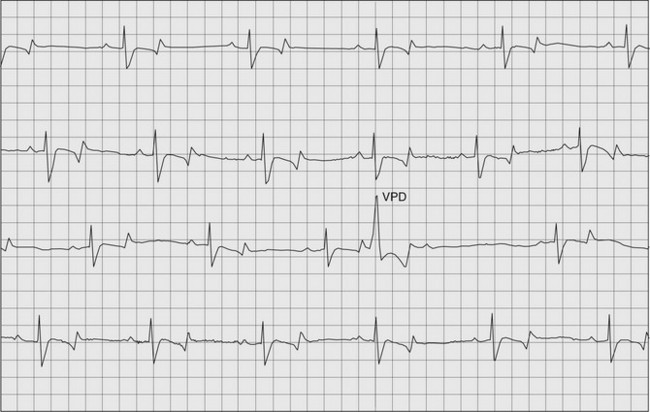
When interpreting resting ambulatory ECGs some dysrhythmias are often found that are of no clinical significance; the prevalence of second degree atrioventricular block (AVB)1 is much higher during ambulatory recordings at rest than during patient-side ECG recording as a result of reduced sympathetic stimulation when the animal is returned to a more natural environment. This is a normal physiological dysrhythmia and should be of no significance if it resolves during light exercise. Occasional ventricular (VPD) and supraventricular premature depolarizations (SVPD) can also be seen on resting ambulatory recordings and provided that they occur less than 1 per hour and are not present at exercise are not considered abnormal (Figs. 10.1 and 10.2).
AF most frequently presents as a persistent dysrhythmia, but can also present as a paroxysmal form where the dysrhythmia spontaneously resolves. Although resting ambulatory electrocardiography is unlikely to identify this, if not present on a patient-side ECG, horses may have frequent isolated SVPD between episodes. If these are present and the horse has a history of a dysrhythmia following exercise, often associated with a sudden loss of performance,2 then this may support a tentative diagnosis of paroxysmal atrial fibrillation. If isolated SVPD are frequent without a history that supports a diagnosis of paroxysmal atrial fibrillation the horse should undergo a full cardiovascular assessment. Although SVPD are unlikely to destabilize and compromise cardiac function they may be evidence of underlying atrial myocardial disease. ( AF, SFP, VMD)
AF, SFP, VMD)
Frequent VPD (see Fig. 10.2) that are present on an ambulatory resting ECG may be suggestive of underlying myocardial disease or may occur in horses with aortic valve disease and should prompt a thorough investigation in an attempt to document underlying pathology and determine whether treatment is likely to be effective (see Chapter 13). In a study of 38 horses with ventricular dysrhythmias, 14 had frequent VPD and were managed by pasture rest and the administration of corticosteroids based on a presumptive diagnosis of myocarditis. There was an improvement of dysrhythmia frequency in nine horses, in five of which the dysrhythmia was completely abolished suggesting that these dysrhythmias represent underlying myocardial pathology (Bowen IM, Marr CM, unpublished observations). Frequent or complex VPD are reported to be associated with sudden cardiac death in humans3 and horses4 and it is believed that they persist or deteriorate in horses that are kept in exercise. Therefore, rest is an important aspect of management of these animals and glucocorticoids are sometimes recommended in the belief that the period of rest required would be shorter. Where horses have frequent isolated ventricular premature complexes their prevalence should be evaluated during exercise. Although isolated single VPD have little effect on cardiac output, they may become more frequent with exercise or result in ventricular tachycardia, which could result in collapse during exercise or even sudden death should ventricular tachycardia develop into ventricular fibrillation. ( AF, AR, RCT)
AF, AR, RCT)
Ventricular tachycardia is most likely to be seen in the critical care setting with the use of ambulatory or telemetric electrocardiography (see Chapter 21). There is a particular association between horses with gastrointestinal tract disease and ventricular dysrhythmias, and electrocardiography should be considered when heart rates are higher than would be expected for the degree of pain and hypovolaemia.5 These dysrhythmias may represent changes in electrolyte, acid-base or fluid status or endotoxaemia and therefore an assessment of the underlying cause is important. Cardiac troponin I concentrations may be increased in horses undergoing exploratory laparotomy for the correction of strangulating small intestinal lesions. This suggests a degree of cardiac myocyte damage, which in one study was shown to be related to hypovolaemia rather than endotoxaemia.6 Therefore, volume expansion should be considered in these animals. Criteria for diagnosis and specific management of ventricular dysrhythmias are detailed in Chapter 13. The aim of diagnosis, management and monitoring of these animals is to identify those at risk from progression to ventricular fibrillation which is rarely amenable to intervention.
EXERCISING AMBULATORY ELECTROCARDIOGRAPHY
Exercising electrocardiography can be used to assess the significance of dysrhythmias detected at rest and to identify dysrhythmias that were otherwise undetected and that only occur during exercise. The advantage of ambulatory electrocardiography in this setting is that the animal can be examined in the same conditions that provoke clinical signs. Exercising ambulatory electrocardiography is indicated for investigation of horses that are presented for investigation of poor performance and collapse and should form part of the evaluation of a horse with aortic valve regurgitation. In addition to providing information about cardiac rhythm cardiac rate can be obtained and can be compared to speed of the horse at the time using either a high-speed treadmill or GPS-based velocity devices. Further details regarding exercise testing and interpretation of exercising electrocardiography can be found in Chapter 11.
HEART RATE VARIABILITY
Heart rate is not static, even in the resting horse, and changes in beat-to-beat intervals occur in the normal healthy animal. As such, the classical view of the heart possessing a metronome-like character only applies to the decentralized heart. In vivo the heart is under the influence of both the autonomic nervous system and the neuroendocrine system in order to maintain normal arterial blood pressure and result in cyclical changes in heart rate (R–R intervals). Techniques of assessing heart rate variability therefore quantify neurohormonal control and do so independently of heart rate providing an indicator of cardiovascular well being. The greater the heart rate variability, the healthier the heart. For example, both respiratory sinus arrhythmia and second degree atrioventricular block are considered normal physiological dysrhythmias1,7 and are a result of autonomic control of the heart.
Determination of heart rate variability
Heart rate variability can be determined from a recorded ECG by extraction of normal R–R intervals (termed N–N intervals; normal–normal) either manually or automatically. These data can then be used to create a tachogram of R–R data (Fig. 10.3) and used for subsequent analysis. The duration of recording and environment in which the recording is made is important to consider. Most heart rate variability indices are obtained from continuous ambulatory recordings where the influence of external stimuli such as handling and transport can be excluded while providing large amounts of data that can be analysed. Accurate detection of normal intervals is essential and therefore the quality of ECG recording is vital in calculating accurate heart rate variability indices. The author’s recommendations for obtaining ECG recordings for heart rate variability analysis are shown in Table 10.1.
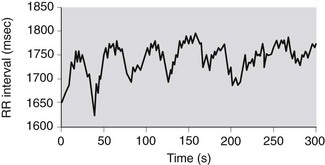
Figure 10.3 Tachogram of normal R–R (N–N) intervals from a horse showing cyclic fluctuations in heart rate.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


