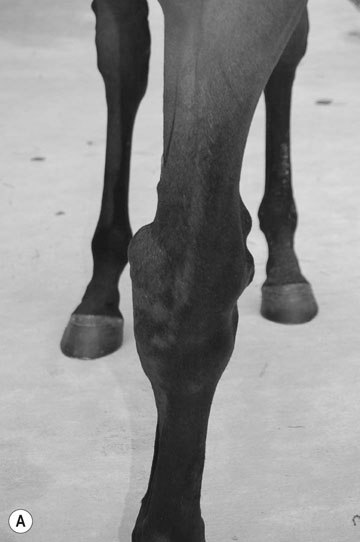
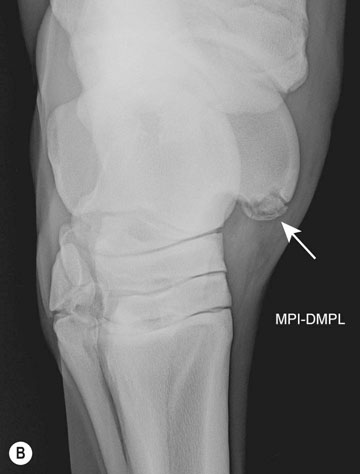
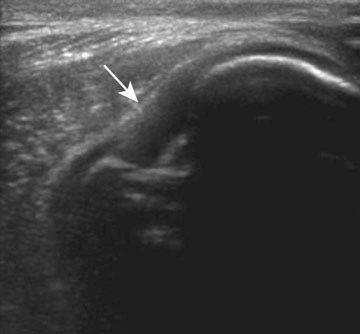
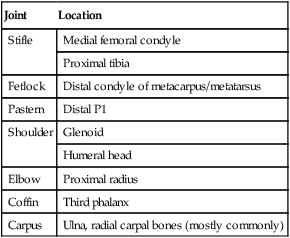
• The defects are usually obvious at birth but many may show remarkable improvement over the early weeks of life. • Radiography can help confirm suspected lesions and further evaluate the degree and severity of the lesion. • Treatment usually consists of conservative management with many mild cases improving. Severe cases or cases with multiple defects may require euthanasia. • Clinical examination and radiographs. • Radiographic changes are often marked but in some cases may appear minimal and the interpretation of the radiographic appearance may be particularly difficult as a result of both the technical difficulty of obtaining suitable projections and the immaturity of the centers of ossification. • Cases in which joints are completely fused, having no mobility at all or those with contractions greater than 90° have a poor prognosis. The grade of incomplete ossification may be appreciated by radiographic examination: Grade 1. Some cuboidal bones with no ossification Grade 2. All cuboidal bones had radiographic evidence of some ossification Grade 3. Cuboidal bones are small and round with consequent ‘wide’ appearance of the joint spaces Grade 4. Cuboidal bones are shaped like the adult counterparts. • Radiographic examination to assess degree of ossification, extent of bone compression and some cases may have concurrent infections. Assessment of white cell count and fibrinogen if there is any doubt about whether there may be a septic element. • Foals should be restricted from excessive exercise to prevent compression of the tarsal cuboidal bones and slowly reintroduced to normal turnout even after complete ossification has occurred. • The tarsus should be radiographed every 10–14 days. If sepsis is suspected based on blood work and radiographic findings, foals should also be started on broad-spectrum antibiotics. • Once collapse of the tarsal or carpal bones has occurred, the condition is easily recognized clinically by the abnormal angles adopted by the affected limb(s). Concurrent flexural deformities and other developmental defects may be found in some cases. Prognosis is usually poor for severe cases. • Clinical examination and radiographs to confirm and assess trochlear ridges. • Medical management consisting of exercise restriction and manual replacement of the patella can be used as treatment in intermittent unilateral cases. • Surgical correction is generally recommended for more persistent luxations or for foals with difficulty ambulating. A number of different surgical procedures can be used individually or combined depending on the severity of the case and surgeon preference. • Palpation of the costochondral junctions during physical exam can sometimes identify fractured ribs. • The fractured ribs themselves can be well-visualized with ultrasound, even when non-displaced, and the technique requires less positioning and manipulation of the injured patient than does radiography. Ultrasound can also be used to determine the degree of fracture segment displacement and the proximity of bone ends to the heart. • Four to six weeks are considered to be necessary for stabilization of the thoracic wall following rib fractures. Foals are normally box rested for 2–3 weeks and then reassessed ultrasonographically before commencing paddock turnout. Administration of analgesics is generally avoided as some pain limits movement and helps avoid additional displacement of fracture segments as a result of exercise. • The formation of a hematoma or thrombus at the broken bone ends is typical of a rib fracture injury in the acute stages. Serial examinations document the evolution of this finding to bony callus formation, and eventual smoothing and remodeling of the callus with time. • Deformation of the lung surface and thickening of the visceral pleura may be semi-permanent to permanent findings in the long-term assessment of these foals. • Foals that have severely displaced fractures that are adjacent to the heart or causing significant pulmonary contusions are considered surgical candidates. Osteochondrosis commonly occurs in the tarsus, stifle and fetlock joints. Though uncommon, osteochondrosis can occur in the scapulohumeral, elbow and hip joints. Tables 7.1 and 7.2 list the most common locations of lesions within each joint. Lesions can potentially regress. In the hock, 5 months has been used as a possible cut off for lesions regressing. After 5 months, lesions will typically not regress. In the stifle, 8 months is the cut off for a lesion regression involving the lateral trochlear ridge. Table 7.1 Osteochondritis dissecans (OCD) Reproduced from McAuliffe SB, Slovis NM (eds) Color Atlas of Diseases and Disorders of the Foal (2008), with permission from Elsevier. Table 7.2 Reproduced from McAuliffe SB, Slovis NM (eds) Color Atlas of Diseases and Disorders of the Foal (2008), with permission from Elsevier. • Diagnosis of osteochondritis is often easily made based on signalment, history, clinical signs and radiographic findings. Ultrasound examination of affected joints can also help to evaluate and confirm the presence of a cartilaginous flap. • Treatment of osteochondral lesions involves conservative or surgical management. Conservative management involves limiting exercise and chondroprotective therapy and is indicated in young foals and those which do not have any effusion or lameness associated with their OCD lesion(s). • Surgical management of osteochondritis dissecans typically involves surgical debridement of the fragment and the fragment bed. Surgical management of subchondral bone cysts has included debridement, cartilage replacement, packing the cyst with bone marrow or injection of corticosteroids. Surgical treatment should be considered for foals with joint effusion and lameness. Prophylactic removal may also be considered in young horses intended for sale. • Fetlock. Many fetlock lesions can improve radiographically over time with conservative management. Surgical treatment should be considered only in foals that demonstrate joint effusion and lameness. Lesions of the palmar/plantar aspect of P1 do not often require surgery. • Hock (tarsus). The distal intermediate ridge of the tibia is the most common site of lesions and these are rarely associated with effusion and lameness. Lesions of the medial malleolus are more likely to result in joint effusion and lameness requiring surgical treatment. Lesions of the lateral trochlear ridge can be quite variable in size but if large may result in effusion and lameness. Most medial trochlear ridge lesions are incidental findings and do not require treatment. • Shoulder and elbow. OCD lesions of the shoulder and elbow are normally only recognized when associated with lameness. The lameness in these cases may develop insidiously or acutely and identifiying the site of the lesion is often difficult. Surgery should only be considered in foals less than 8–10 months of age if they are intractably lame as some cases may improve with rest. Radiography may also underestimate the size of the lesions making pre-surgical assessments of future athletic function difficult.
Skeletal disorders
Developmental disorders
Deformities of the axial skeleton (Figs. 7.1–7.4)
Deformities of the vertebral column
Diagnosis and treatment
Congenital deformities of the limbs and joints (arthrogryposis) (Figs. 7.6 & 7.7)


Diagnosis and treatment
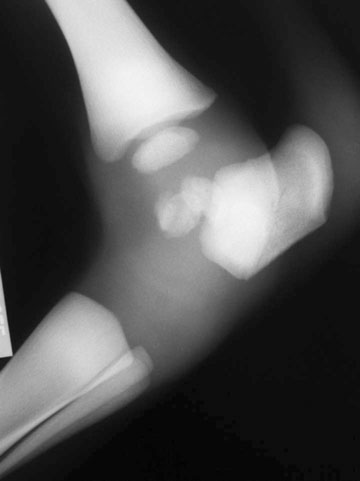
Collapse of carpal and/or tarsal bones and incomplete ossification (Figs. 7.8–7.11)
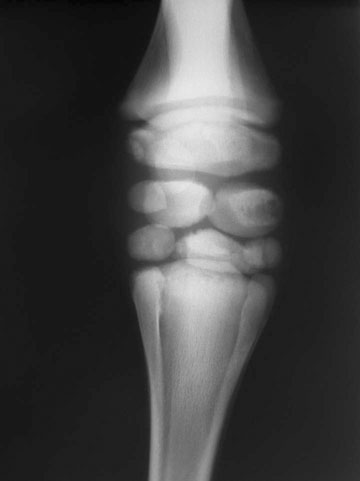




Diagnosis and treatment
Congenital luxation of the patella (Fig. 7.12)

Diagnosis and treatment
Fractured ribs (Figs. 7.13–7.16)
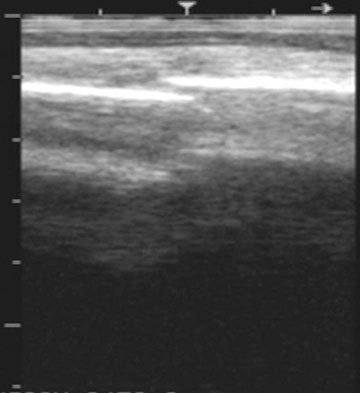
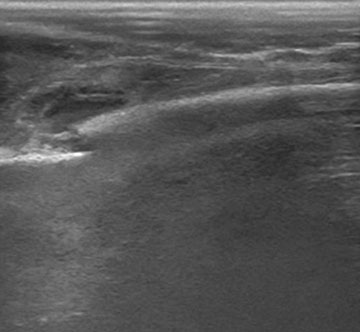

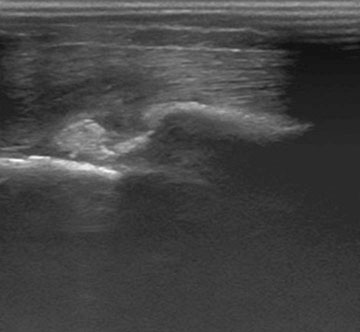
Diagnosis
Treatment
Hereditary multiple exostoses (multiple osteochondroma, multiple cartilagenous exostosis, diaphyseal aclasis or endochondromatosis) (Fig. 7.17)

Developmental disorders: Acquired conditions
Osteochondrosis (Figs. 7.18–7.24)




Joint
Location
Fetlock
Mid-sagittal ridge
Dorsal proximal medial/lateral P1
Palmar/plantar P1
Tarsus
Distal intermediate ridge of tibia
Medial malleolus
Lateral trochlear ridge
Medial trochlear ridge
Stifle
Lateral trochlear ridge
Medial trochlear ridge
Distal aspect of patella
Shoulder
Glenoid cavity
Humeral head
Elbow
Lateral/medial humeral condyle (uncommon)

Joint
Location
Stifle
Medial femoral condyle
Proximal tibia
Fetlock
Distal condyle of metacarpus/metatarsus
Pastern
Distal P1
Shoulder
Glenoid
Humeral head
Elbow
Proximal radius
Coffin
Third phalanx
Carpus
Ulna, radial carpal bones (mostly commonly)
Diagnosis and treatment
Prognosis
Angular limb deformities (Figs. 7.25–7.28)


![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Skeletal disorders