Chapter 4 THE FORELIMB
As with the previous two chapters, any part of the limb may be involved in surface trauma with bruising and hemorrhage requiring cleaning, disinfection and debridement. Luckily, most of the important structures are on the medial aspect of the limbs and are therefore protected, in most instances, from such damage.
The elbow joint can be a site of several important clinical conditions. The anconeal process of the ulna fits into the olecranon fossa of the humerus and therefore the joint can only dislocate when the joint is in full flexion or when fracture of the humeral epicondyle occurs (repaired by surgery and use of screws). This usually occurs in traumatic accidents. It can also be put back in place with full flexion of the joint. The anconeal process has occasionally a separate centre of ossification from that of the olecranon. In this case, the anconeal process detaches following trauma or fails to unite and is pulled off by M. triceps and may have to be removed surgically. Caudolateral arthrotomy of the elbow is used to remove an anconeal process that is disunited. A curved incision is made over the distal third of the humerus to the proximal third of the radius. The pronator teres and the flexor carpi radialis are then separated to expose the joint capsule.

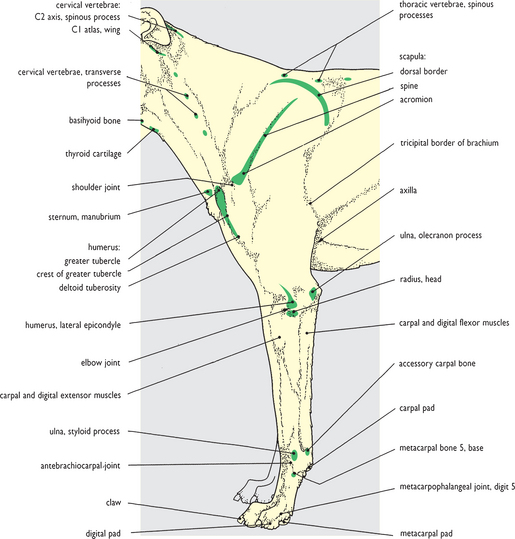
Fig. 4.1 Surface features of the neck and forelimb: left lateral view. The palpable bony prominences of the neck and forelimb are shown. In addition the trachea is clearly palpable on the underside of the neck. ‘Soft’ structures identifiable include the mandibular lymph nodes at the cranial end of the neck and the superficial cervical nodes in front of the scapula at the caudal end. A pulse may be detected in the common carotid artery in the neck, but also from the brachial/median artery in the cubital fossa on the flexor surface of the elbow joint. The external jugular vein may be raised by pressure in the jugular fossa: the cephalic vein may also be raised in the antebrachium by pressure immediately distal to the elbow joint. Fig. 4.1A at the foot of the page shows the main topographical regions that are recognized for descriptive purposes. The boundaries of regions in the neck are a trifle arbitrary because of the absence of discernible underlying features. The four main topographical regions of the forelimb are based on internal osteological components; the subsidiary topographical regions are related to the underlying joints between segments.
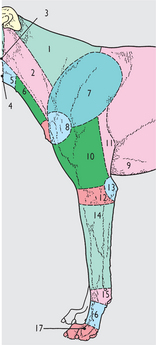
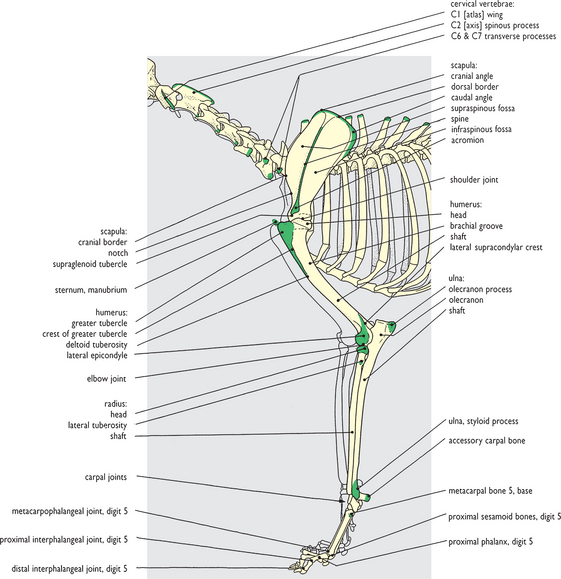
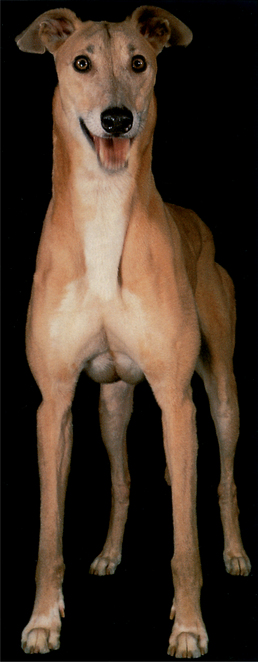
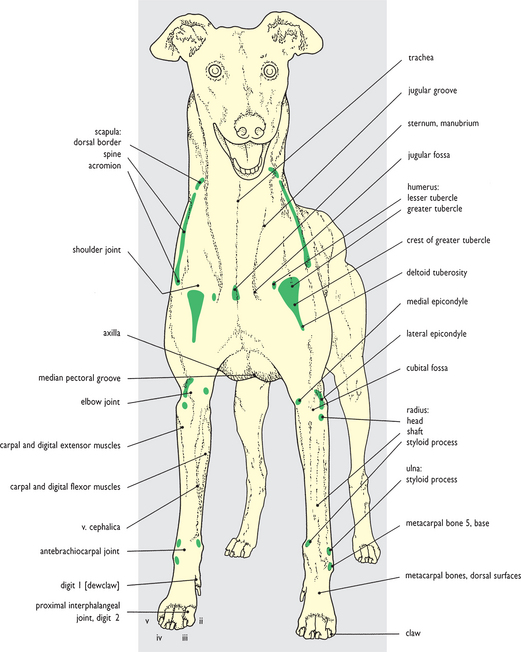
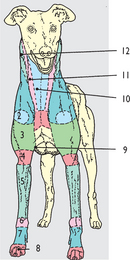

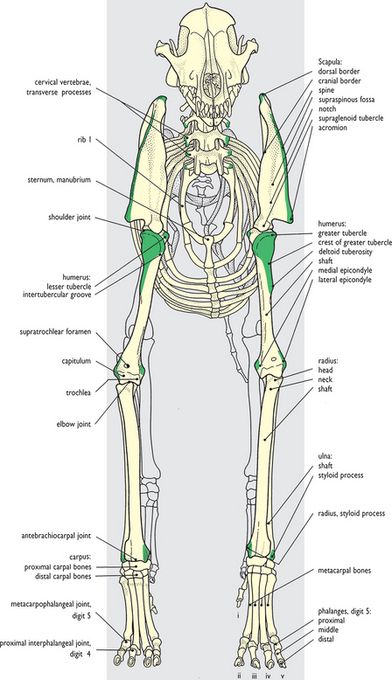
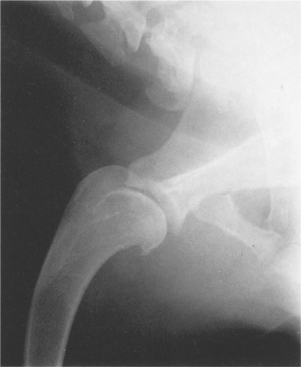

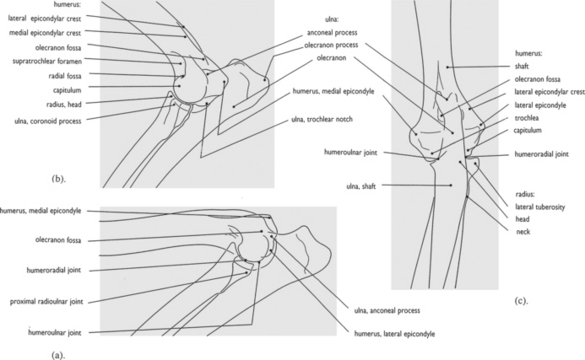

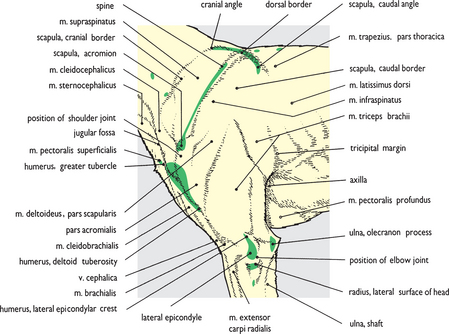
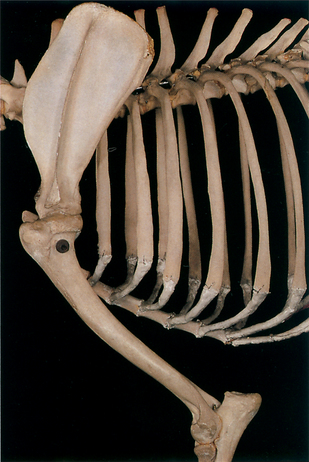
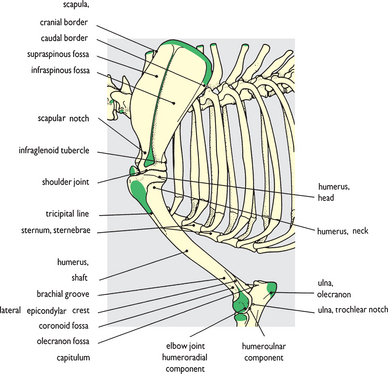
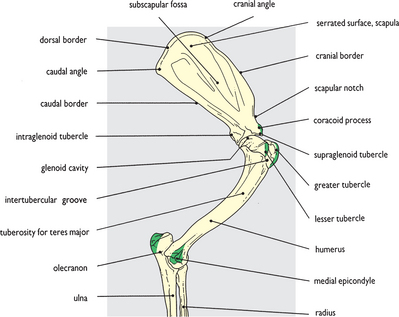
Fig. 4.8 Skeleton of the shoulder and brachium: left lateral view. The features colored green correspond to the palpable bony features shown in the previous figure (Fig. 4.7).

< div class='tao-gold-member'>




