The Forelimb
 . Approach to the Proximal Shaft of the Humerus
. Approach to the Proximal Shaft of the Humerus
 . Approach to the Midshaft of the Humerus Through a Craniolateral Incision
. Approach to the Midshaft of the Humerus Through a Craniolateral Incision
 . Approach to the Shaft of the Humerus Through a Medial Incision
. Approach to the Shaft of the Humerus Through a Medial Incision
 . Minimally Invasive Approach to the Shaft of the Humerus
. Minimally Invasive Approach to the Shaft of the Humerus
 . Approach to the Distal Shaft of the Humerus Through a Craniolateral Incision
. Approach to the Distal Shaft of the Humerus Through a Craniolateral Incision
 . Approach to the Distal Shaft and Supracondylar Region of the Humerus Through a Medial Incision
. Approach to the Distal Shaft and Supracondylar Region of the Humerus Through a Medial Incision
 . Approach to the Lateral Aspect of the Humeral Condyle and Epicondyle in the Dog
. Approach to the Lateral Aspect of the Humeral Condyle and Epicondyle in the Dog
 . Approach to the Lateral Aspect of the Humeral Condyle and Epicondyle in the Cat
. Approach to the Lateral Aspect of the Humeral Condyle and Epicondyle in the Cat
 . Approach to the Lateral Humeroulnar Part of the Elbow Joint
. Approach to the Lateral Humeroulnar Part of the Elbow Joint
 . Approach to the Supracondylar Region of the Humerus and the Caudal Humeroulnar Part of the Elbow Joint
. Approach to the Supracondylar Region of the Humerus and the Caudal Humeroulnar Part of the Elbow Joint
 . Approach to the Humeroulnar Part of the Elbow Joint by Osteotomy of the Tuber Olecrani
. Approach to the Humeroulnar Part of the Elbow Joint by Osteotomy of the Tuber Olecrani
 . Approach to the Humeroulnar Part of the Elbow Joint by Tenotomy of the Triceps Tendon
. Approach to the Humeroulnar Part of the Elbow Joint by Tenotomy of the Triceps Tendon
 . Approach to the Elbow Joint by Osteotomy of the Proximal Ulnar Diaphysis
. Approach to the Elbow Joint by Osteotomy of the Proximal Ulnar Diaphysis
 . Approach to the Head of the Radius and Lateral Parts of the Elbow Joint
. Approach to the Head of the Radius and Lateral Parts of the Elbow Joint
 . Approach to the Head of the Radius and Humeroradial Part of the Elbow Joint by Osteotomy of the Lateral Humeral Epicondyle
. Approach to the Head of the Radius and Humeroradial Part of the Elbow Joint by Osteotomy of the Lateral Humeral Epicondyle
 . Approach to the Medial Humeral Epicondyle
. Approach to the Medial Humeral Epicondyle
 . Approach to the Medial Aspect of the Humeral Condyle and the Medial Coronoid Process of the Ulna by an Intermuscular Incision
. Approach to the Medial Aspect of the Humeral Condyle and the Medial Coronoid Process of the Ulna by an Intermuscular Incision
 . Approach to the Medial Aspect of the Humeral Condyle and the Medial Coronoid Process of the Ulna by Osteotomy of the Medial Humeral Epicondyle
. Approach to the Medial Aspect of the Humeral Condyle and the Medial Coronoid Process of the Ulna by Osteotomy of the Medial Humeral Epicondyle
 . Approach to the Proximal Shaft and Trochlear Notch of the Ulna
. Approach to the Proximal Shaft and Trochlear Notch of the Ulna
 . Approach to the Tuber Olecrani
. Approach to the Tuber Olecrani
 . Approach to the Distal Shaft and Styloid Process of the Ulna
. Approach to the Distal Shaft and Styloid Process of the Ulna
 . Approach to the Head and Proximal Metaphysis of the Radius
. Approach to the Head and Proximal Metaphysis of the Radius
 . Approach to the Shaft of the Radius Through a Medial Incision
. Approach to the Shaft of the Radius Through a Medial Incision
 . Approach to the Shaft of the Radius Through a Lateral Incision
. Approach to the Shaft of the Radius Through a Lateral Incision
 . Approach to the Distal Radius and Carpus Through a Dorsal Incision
. Approach to the Distal Radius and Carpus Through a Dorsal Incision
 . Approach to the Distal Radius and Carpus Through a Palmaromedial Incision
. Approach to the Distal Radius and Carpus Through a Palmaromedial Incision
 . Approach to the Accessory Carpal Bone and Palmarolateral Carpal Joints
. Approach to the Accessory Carpal Bone and Palmarolateral Carpal Joints
 . Approaches to the Metacarpal Bones
. Approaches to the Metacarpal Bones
 . Approach to the Proximal Sesamoid Bones
. Approach to the Proximal Sesamoid Bones
 . Approaches to the Phalanges and Interphalangeal Joints
. Approaches to the Phalanges and Interphalangeal JointsApproach to the Proximal Shaft of the Humerus
Alternative Approach
Medial exposure of the proximal shaft of the humerus is obtained with the approach to the craniomedial region of the shoulder (see Plate 30). For greater exposure distally, the cephalic vein is ligated where it disappears under the caudal edge of the brachiocephalicus muscle. The insertions of superficial pectoral and deep pectoral muscles are incised along their entire lengths on the humerus.
Description of the Procedure
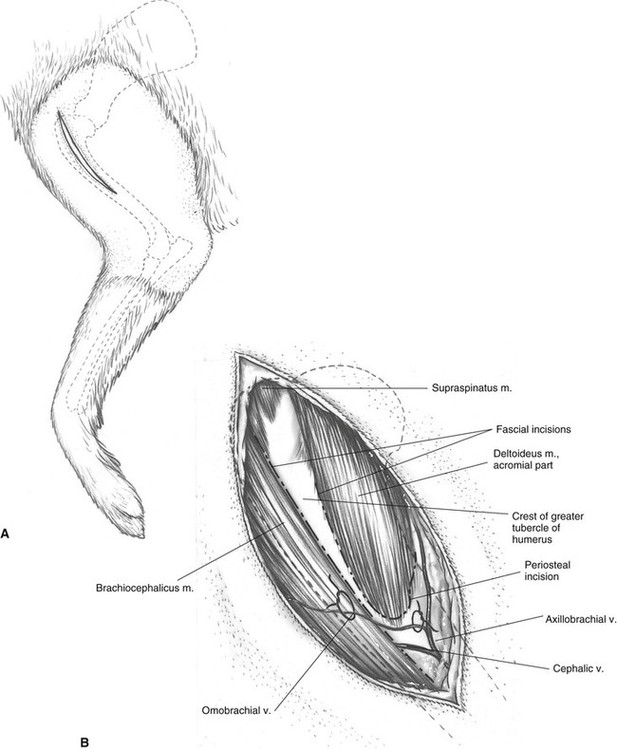
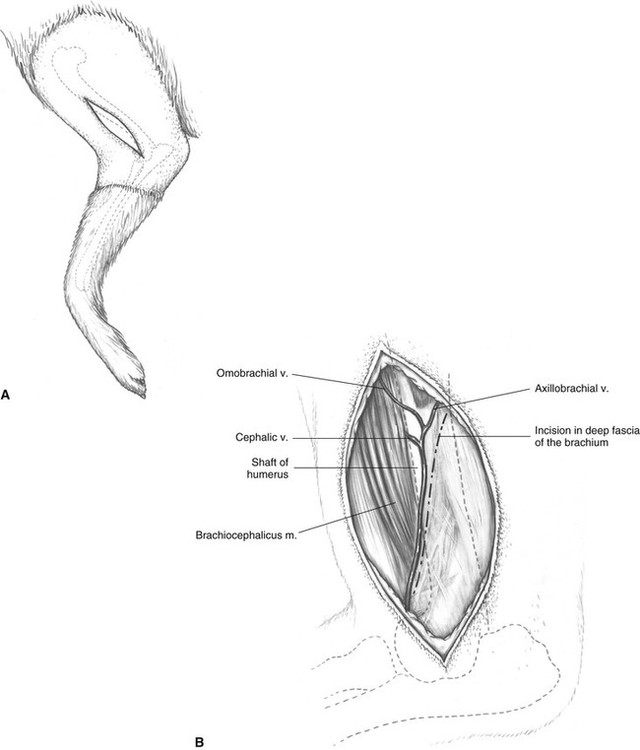
A Identify the acromion process, greater tubercle of the humerus, and deltoid tuberosity by palpation. The skin incision is made slightly lateral to the cranial midline of the bone and extends from the greater tubercle of the humerus distally to a point near the midshaft of the bone, just beyond the deltoid tuberosity.
B Following undermining and retraction of the skin, an incision is made through the deep fascia along the lateral border of the brachiocephalicus muscle. The insertion of the acromial part of the deltoideus muscle is also incised.
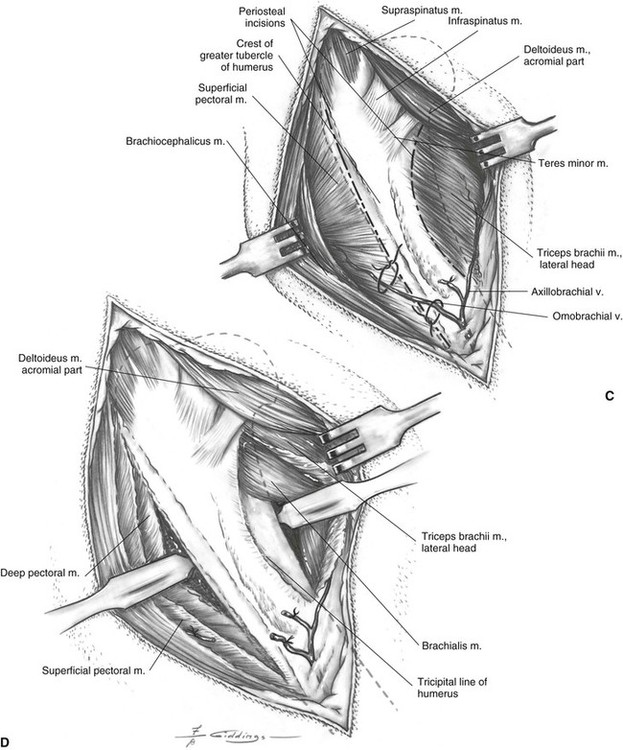
C The brachiocephalicus can be retracted cranially following blunt dissection between the muscle and the bone. The deltoideus muscle is retracted caudally to reveal the tendons of insertion of the teres minor and infraspinatus muscles. If more exposure of bone is needed, the insertions of the superficial pectoral muscle and the lateral head of the triceps muscle can be incised.
D Periosteal elevation of the lateral head of the triceps exposes the lateral and caudal aspects of the shaft. If the craniomedial shaft must be exposed, a portion of the insertion of the deep pectoral muscle can be elevated. This muscle insertion is just medial to that of the superficial pectoral muscle.
Additional Exposure
Proximal extension of this approach to the cranial region of the shoulder, with osteotomy of the greater tubercle of the humerus, provides total exposure of the scapular neck and most of the glenoid cavity (see Plate 32).
Medial extension of this approach to the craniomedial region of the shoulder (see Plate 30) provides exposure of the tendon of origin of the biceps brachii muscle, supraglenoid tuberosity, and medial aspect of the humeral head.
Distal extension of this approach to the shaft of the humerus, through a craniolateral incision (see Plate 34), provides good exposure of the proximal two thirds of the humerus.
The entire length of the humerus is exposed from the craniolateral aspect by the combination of the craniolateral approaches to the proximal (see Plate 33), middle (see Plate 34), and distal (see Plate 37) portions of the humerus. The brachialis muscle and radial nerve cover the humeral shaft distally and need to be protected and retracted.
Closure
The deep pectoral and triceps muscles are not reattached because they are only partially elevated and will reattach to the periosteum by fibrosis. The external fasciae of the superficial pectoral and deltoideus muscles are sutured to each other over the cranial border of the bone. The deep fascia is reattached to the edge of the brachiocephalicus muscle, followed by closure of the subcutaneous tissues and skin.
Approach to the Midshaft of the Humerus Through a Craniolateral Incision
Alternative Approach
The approach to the shaft of the humerus through a medial incision is an alternative (see Plate 35). It provides exposure of the entire diaphysis of the humerus that may be valuable for bone plate application.
Description of the Procedure
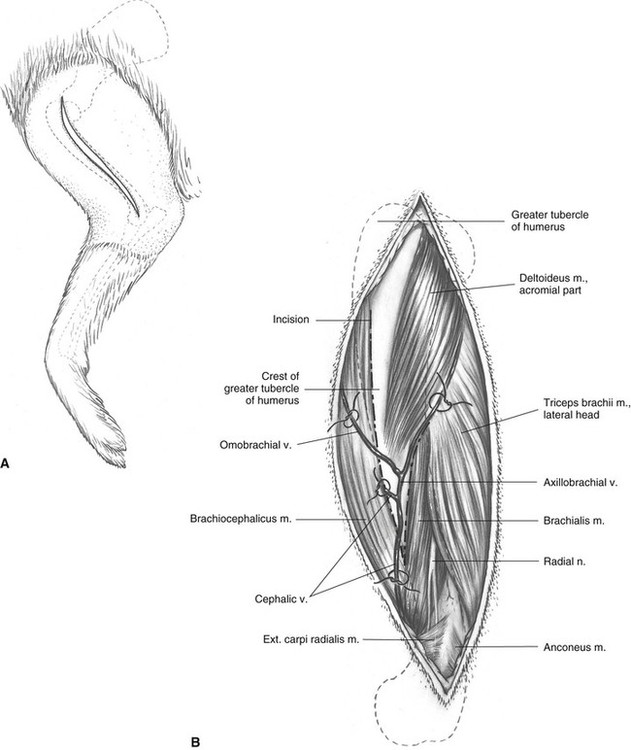
A Palpate the greater tubercle, deltoid tuberosity, and lateral epicondyle of the humerus. The skin incision extends from the greater tubercle of the humerus proximally to the lateral epicondyle distally, following the craniolateral border of the humerus.
B Subcutaneous fat and fascia are incised on the same line and mobilized and retracted with the skin. Fat and brachial fascia are incised and dissected away to allow visualization of the cephalic vein. Brachial fascia is incised along the lateral border of the brachiocephalicus muscle and distally over the cephalic vein.
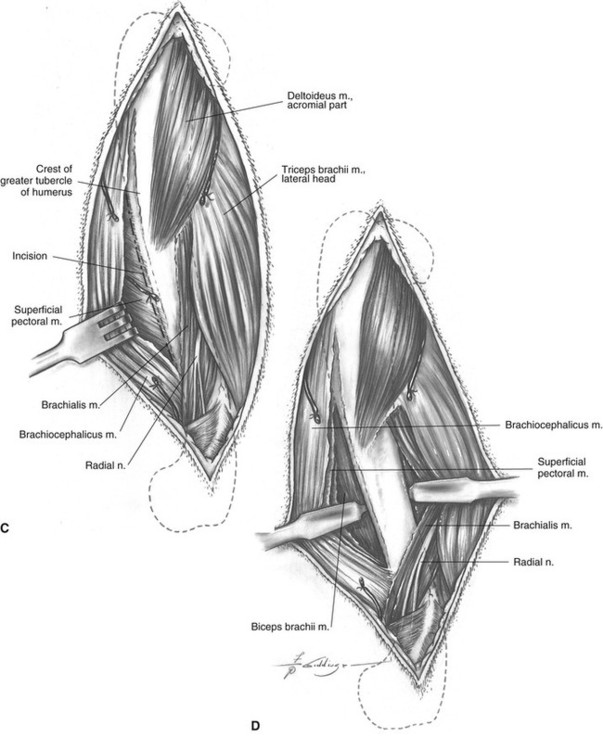
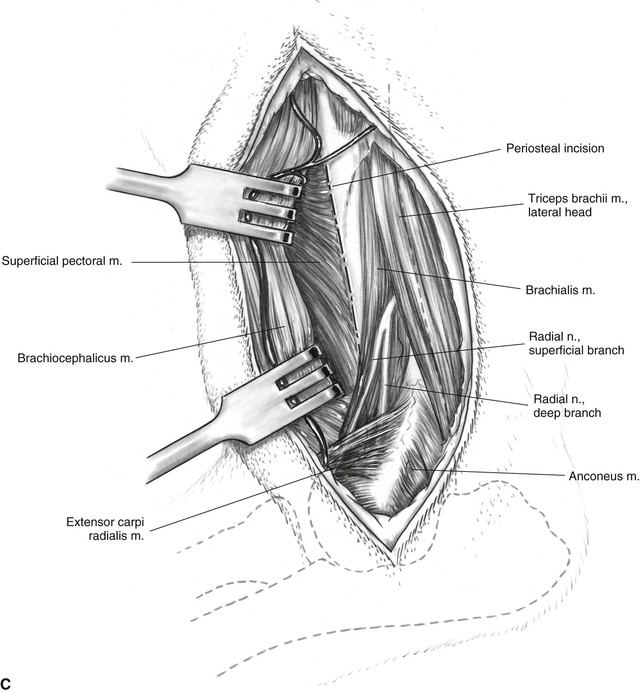
C An incision is next made in the periosteal insertion of the superficial pectoral and brachiocephalicus muscles on the humeral shaft. The radial nerve overlying the brachialis muscle should be identified and protected when making these incisions.
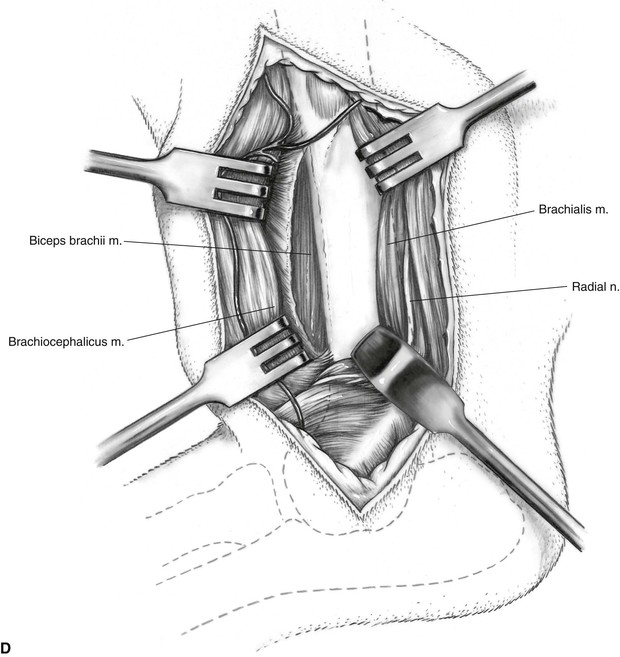
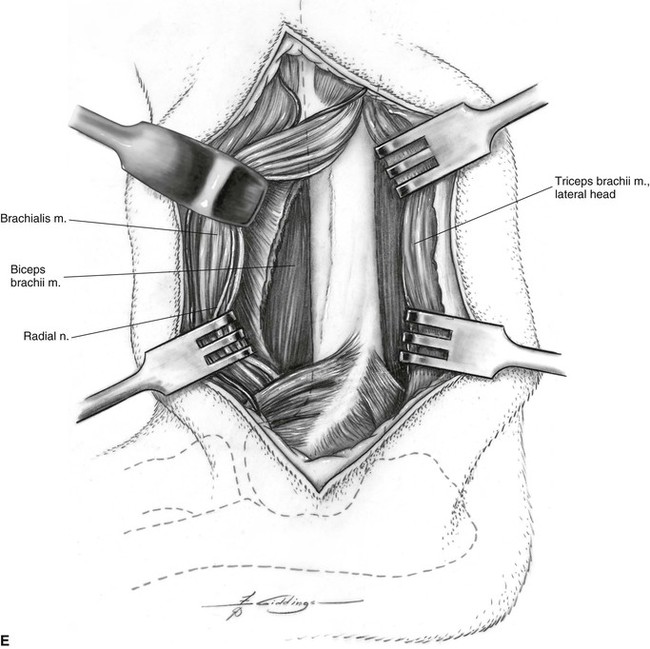
D Hohmann retractors are used to retract the brachialis and triceps muscles caudally and expose the musculospiral groove of the humerus. Cranial retraction will elevate the biceps brachii, superficial pectoral, and brachiocephalicus muscles from the shaft. Again, the radial nerve must be protected during retraction. Avoid continuation of dissection farther distally between the brachialis and brachiocephalicus muscles because the superficial branch of the radial nerve may be inadvertently damaged. For additional exposure of the humerus distally, retract the brachialis muscle and radial nerve cranially (see Plate 37E).
Additional Exposure
Based on a procedure of Wallace and Berg,51 and a procedure of Newton.31 Greater visualization of the distal shaft of the humerus can be obtained by transection of the brachialis muscle, with the transected muscle being used as a physiologic retractor of the radial nerve, its preservation being paramount.
Extension of this approach more proximally with subperiosteal elevation of the acromial head of the deltoideus muscle (see Plate 33) provides good exposure of the proximal two thirds of the humerus.
More distal exposure of the humeral shaft can be obtained by cranial retraction of the brachialis muscle and radial nerve (see Plate 37E).
The entire length of the humerus is exposed by the combination of the craniolateral approaches to the proximal (see Plate 33), middle (see Plate 34), and distal (see Plate 37) portions of the humerus. The brachialis muscle and radial nerve cover the humeral shaft distally and need to be protected and retracted.
Approach to the Shaft of the Humerus Through a Medial Incision
Based on a Procedure of Montgomery, Milton, and Mann29
Alternative Approach
This approach through a medial incision allows visualization of the entire shaft of the humerus, which is valuable when applying a bone plate to a highly comminuted fracture. As an alternative, more limited exposure is obtained with the craniolateral approach to the midshaft (see Plate 34), the distal shaft (see Plate 37), or a combination of both. Lateral exposure of the distal one third of the shaft is impaired by the overlying brachialis muscle and radial nerve.
Description of the Procedure
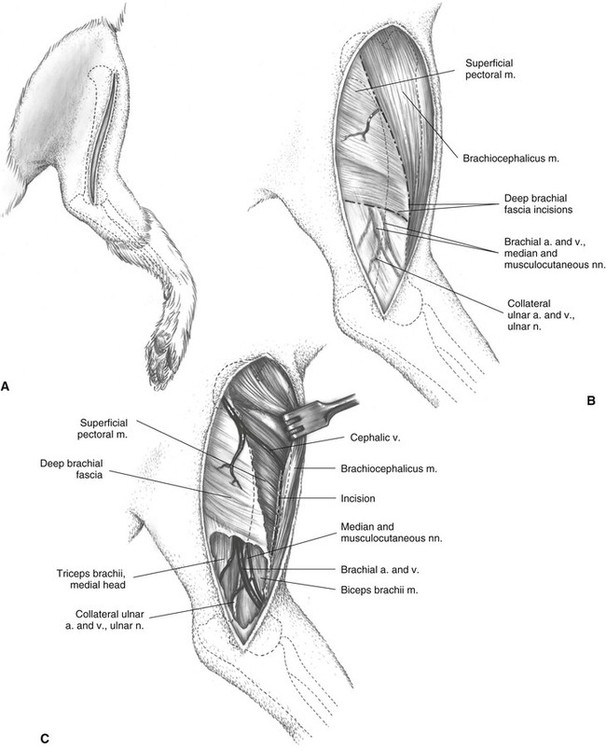
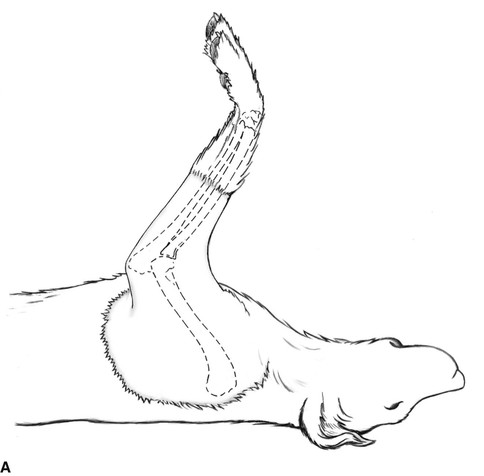
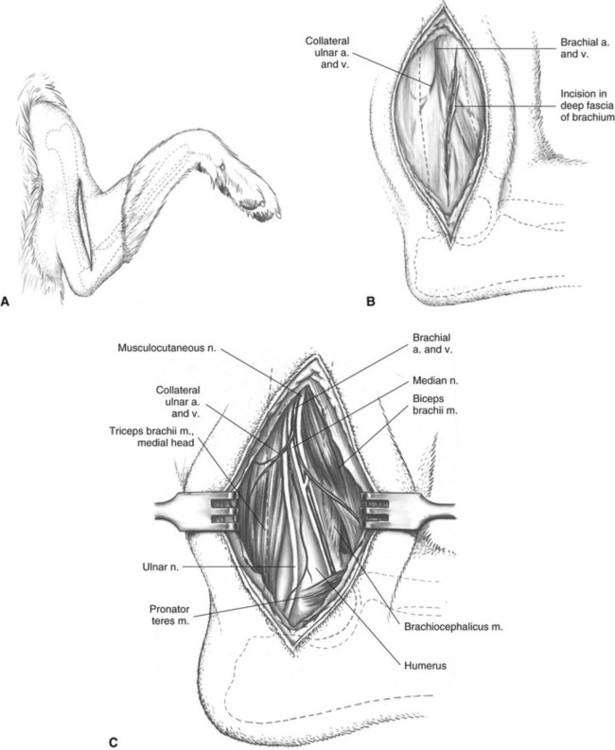
A Identify by palpation the greater tubercle and medial epicondyle of the humerus. The medial skin incision begins proximally at the level of the greater tubercle and extends distally to the medial epicondyle. Subcutaneous fat and fascia are incised on the same line and retracted with the skin.
B Deep brachial fascia is incised along the cranial border of the brachiocephalicus muscle and along the distal border of the superficial pectoral muscle. The distal part of this incision is made carefully to preserve the underlying neurovascular structures.
C Fascia distal to the superficial pectoral muscle is carefully dissected from the vessels and nerves. The brachiocephalicus muscle is retracted cranially to expose the insertion of the superficial pectoral muscle on the shaft of the humerus. This insertion is incised close to the bone, beginning at the distal border of the muscle and extending proximally to the level of the cephalic vein.
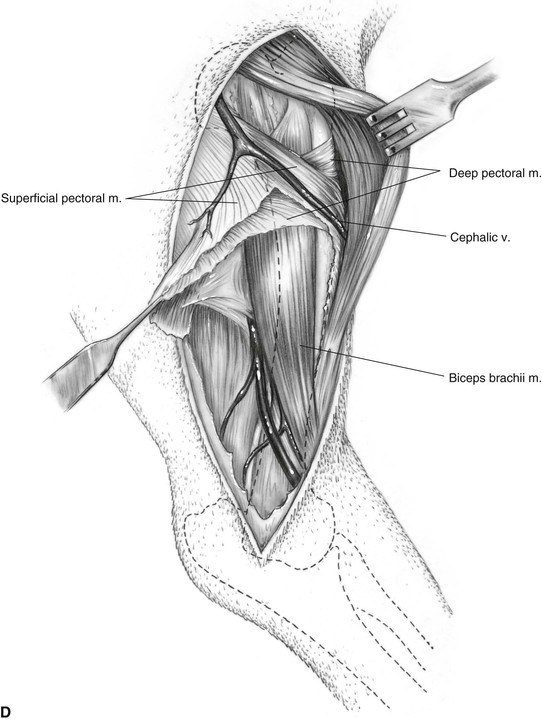
D The superficial pectoral incision is extended into the muscle, parallel to the cephalic vein, by blunt dissection between muscle fibers. The aponeurosis from the superficial part of the deep pectoral muscle is incised along the shaft of the humerus and retracted, exposing the underlying biceps brachii muscle.
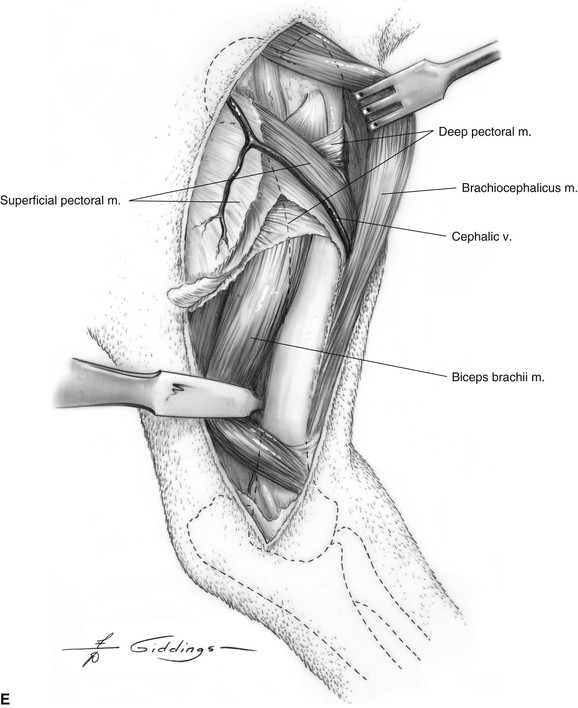
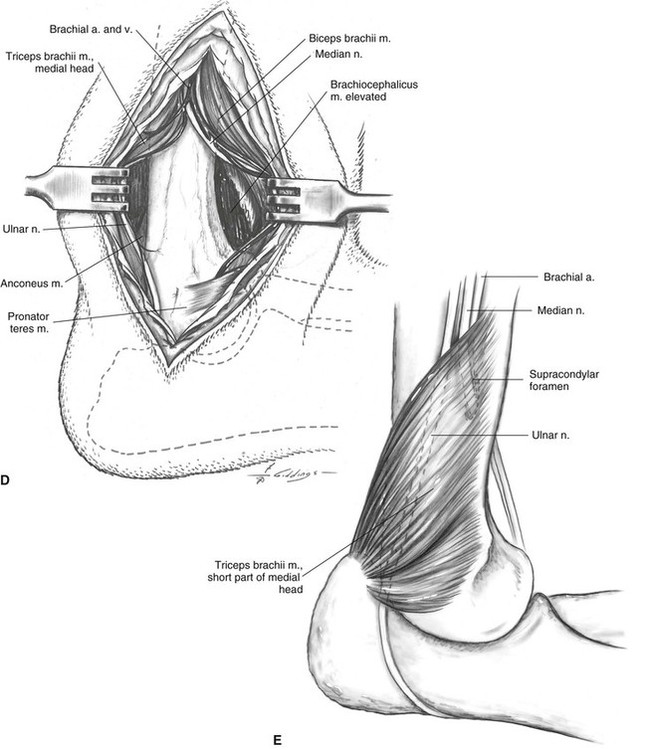
E Exposure of the proximal portion and midportion of the bone is optimal if the brachiocephalicus muscle is retracted cranially and the biceps brachii muscle is retracted caudally. Flexion of the elbow joint will facilitate caudal retraction of the biceps brachii muscle. The remaining attached portion of the superficial pectoral muscle is retracted as necessary, and bone plates are placed under it. If essential, the cephalic vein can be ligated and the entire insertion of the muscle incised.
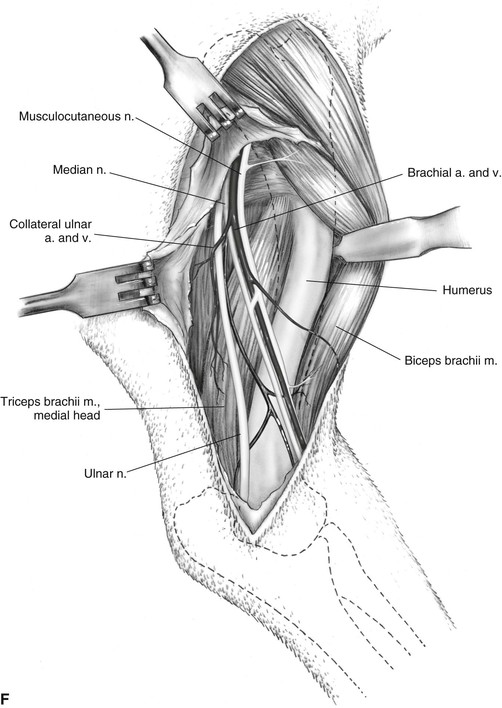
F The middle and distal regions of the humerus are best exposed by cranial retraction of the biceps brachii muscle, which requires careful dissection along the caudal border of the muscle to separate it from the neurovascular structures. The proximal and distal branches of the musculocutaneous nerve must be protected where they penetrate the muscle.
Additional Exposure
More proximal exposure of the intertubercular groove, lesser tubercle, and medial side of the head of the humerus can be obtained by transecting the insertion of the deep pectoral muscle on the greater tubercle (see Plate 32A). The transverse humeral ligament is transected and retraction of the tendon of the biceps brachii muscle from the intertubercular groove is facilitated by flexion of the elbow.
Additional distal exposure is obtained in combination with the approach to the distal shaft and supracondylar region of the humerus through a medial incision (see Plate 38). These two approaches are not completely continuous but are interrupted by the brachial artery and vein and musculocutaneous and median nerves (see Plate 35F). These must be protected and retracted caudally for the midshaft approach (see Plate 35F) and cranially for the more distal exposure (see Plate 38C and D).
Minimally Invasive Approach to the Shaft of the Humerus
Based on a Procedure of Déjardin and Guiot11
Alternative Approach
The alternative minimally invasive approach is a combination of exposure of the craniolateral part of the proximal humerus (Plate 33) with the lateral approach to the humeral condyle and epicondyle (Plate 39). This lateral approach is valuable when applying an interlocking nail, but the contouring of a bone plate to the lateral epicondyle of the humerus is more difficult than it is for the medial epicondyle.
Description of the Procedure
A The patient is positioned in dorsal recumbency with the affected limb suspended for draping. This position permits two orthogonal fluoroscopic images to be obtained before making the surgical approach, as well as during the surgical procedure.
B The limb is abducted, and the distal approach is commenced with a skin incision that is centered over the caudal aspect of the medial epicondyle of the humerus.
C The skin margins are mobilized and retracted. The antebrachial fascia is incised to expose the caudal and distal aspect of the medial epicondyle.
D The medial head of the triceps muscle and the ulnar nerve are mobilized and retracted caudally. The median nerve is not exposed, but care is taken to preserve it. If required, the origin of the superficial digital flexor muscle on the medial epicondylar ridge is partially transected by a few millimeters to expose the distal edge of the bone for intramedullary pin insertion.
E A blunt instrument, such as the soft-tissue retractor illustrated here, is passed along the medial side of the humeral shaft to create an epiperiosteal tunnel. The tunnel is directed toward the craniomedial surface of the proximal part of the humerus.
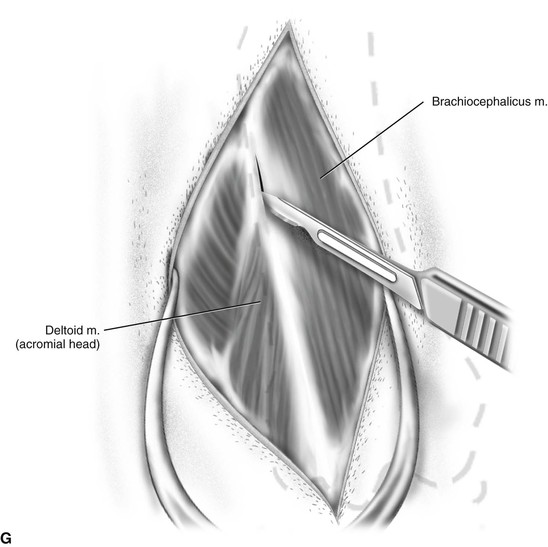
F The second skin incision is made over the craniomedial aspect of the humerus in the region of the insertion of the supraspinatus muscle on the greater tubercle.
G The incision continues through the subcutaneous fat and the fascia along the caudal edge of the brachiocephalicus muscle.
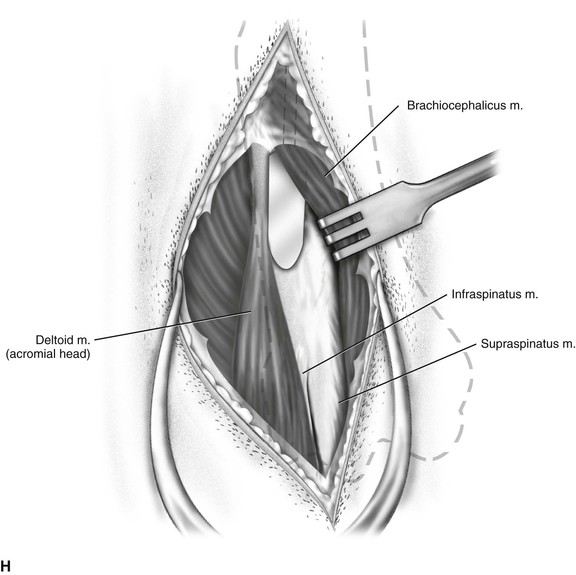
H The brachiocephalicus muscle is retracted medially, and the origin of the superficial pectoral muscle is incised in the proximal region to allow passage of the soft tissue retractor and completion of the epiperiosteal tunnel.
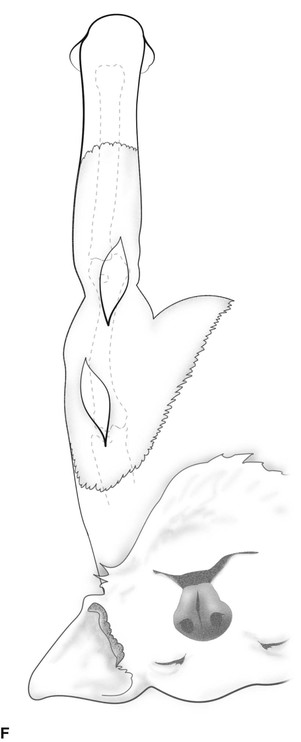
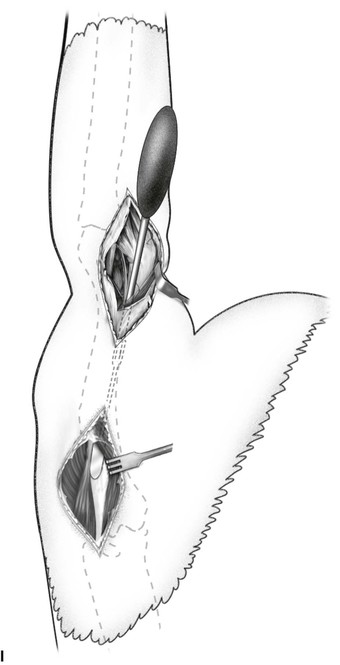
I Overview showing passage of soft tissue retractor from the medial epicondyle to the greater tubercle of the humerus.
Additional Exposure
If necessary, the minimally invasive approach to the humerus can be extended to provide complete exposure of the medial aspect of the humerus (Plate 35).
Closure
The distal incision is closed with sutures placed in the brachial fascia and subcutaneous fat, taking care to avoid injury of the ulnar nerve. The proximal incision is closed by suturing the superficial pectoral muscle to the deltoideus muscle. The external fascia of the brachiocephalicus muscle is sutured to brachial fascia. The subcutaneous tissue and skin are closed in layers.

Approach to the Distal Shaft of the Humerus Through a Craniolateral Incision
Based on a Procedure of Brinker4
Indication
Open reduction of fractures between the midshaft and the supracondylar area of the humerus.
Alternative Approach
The alternative approach through a medial incision to the midshaft (see Plate 35) and distal shaft (see Plate 38) provides exposure to the entire shaft of the humerus, which is valuable when applying a bone plate.
Description of the Procedure
A The craniolateral border of the humerus is the guide for this incision, which commences at the midshaft and ends at the lateral epicondyle.
B The skin margins are mobilized and retracted. Subcutaneous fascia and fat are incised in the same line as the skin, avoiding the cephalic and axillobrachial veins. The deep fascia of the brachium is incised along the cranial border of the triceps. The incision parallels the cephalic and axillobrachial veins to allow their mobilization. The radial nerve must be protected when the distal end of this incision is opened.
C The deep fascia is undermined to allow cranial retraction of the brachiocephalicus muscle and the cephalic vein and exposure of the radial nerve. An incision is made in the periosteal insertion of the superficial pectoral muscle.
D The superficial pectoral muscle is elevated at its insertion on the humerus as necessary to allow cranial retraction. The brachialis muscle is freed from the bone by blunt dissection and is retracted caudally with the triceps and the radial nerve.
E To obtain better exposure of the distal portion of the bone, the lateral head of the triceps brachii muscle can be retracted caudally and the brachialis muscle and radial nerve retracted cranially.
Additional Exposure
Proximal extension of this approach through a craniolateral incision provides exposure to the midshaft (see Plate 34) and proximal shaft (see Plate 33) of the humerus.
Distally this approach can be extended to provide exposure of the lateral aspect of the humeral condyle and epicondyle (see Plate 39) or the lateral humeroulnar part of the elbow joint (see Plate 41).
Precautions
As the radial nerve emerges from under the lateral and accessory heads of the triceps muscle, it provides branches innervating the lateral, medial, and accessory heads of this muscle before coursing laterally over the brachialis muscle. Shortly thereafter it bifurcates into the deep branch that innervates the supinator muscle and all the extensor muscles of the carpus and digits, as well as the superficial branch that provides sensory innervation to the dorsum of the paw.
Approach to the Distal Shaft and Supracondylar Region of the Humerus Through a Medial Incision
Based on a Procedure of Brinker4
Alternative Approaches
The approach to the shaft of the humerus through a medial incision (see Plate 35) is preferred when complete exposure of the midshaft is required.
The approach to the distal shaft of the humerus through a craniolateral incision (see Plate 37) is an alternative, but exposure of the bone is hindered laterally by the overlying radial nerve and brachialis muscle.
Description of the Procedure
A Palpate the greater tubercle and medial epicondyle of the humerus. The skin incision extends from the medial epicondyle proximally along the cranial border of the humerus to the midshaft of the bone.
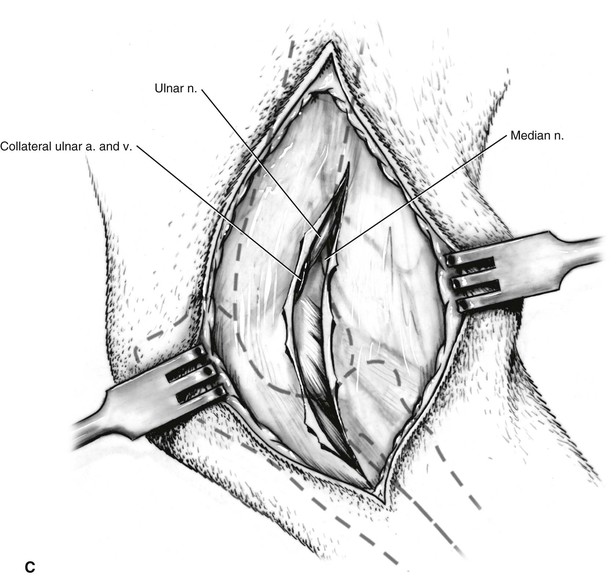
B The skin is retracted and the subcutaneous fat is elevated sufficiently to allow visualization of the brachial and collateral ulnar vessels. The ulnar and median nerves that accompany these vessels are not yet visible; they lie slightly deeper. An incision is made in the deep fascia directly over the distal shaft of the humerus and between the blood vessels. It will be necessary to continue the incision proximally over the vessels.
C Beginning at the medial epicondyle, bluntly dissect the subfascial fat and fascia overlying the humerus to allow initial identification of the ulnar nerve caudally and median nerve cranially.
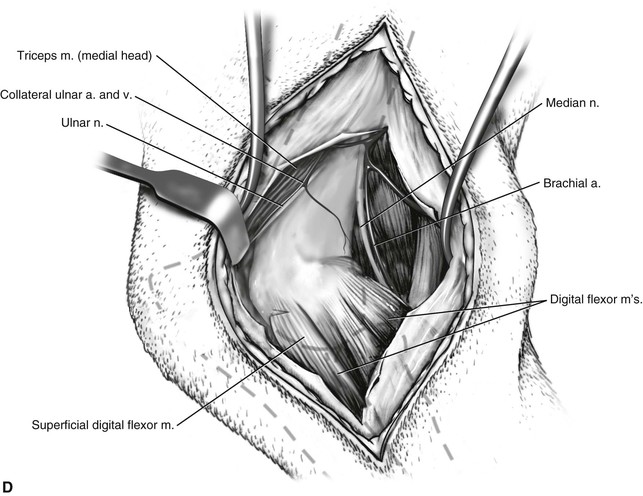
D The manner in which the vessels and the nerves are mobilized depends on the area of the bone that is to be exposed. The method illustrated is used when the distal and supracondylar portions of the humerus are involved. If great care is taken to protect the vessels and nerves, sufficient exposure of the midshaft can be obtained for insertion of the proximal screws in a bone plate. For further exposure of the midshaft of the humerus, the median and musculocutaneous nerves and brachial artery and vein are freed and retracted caudally with the triceps and the collateral ulnar vessels (see Plate 35F).
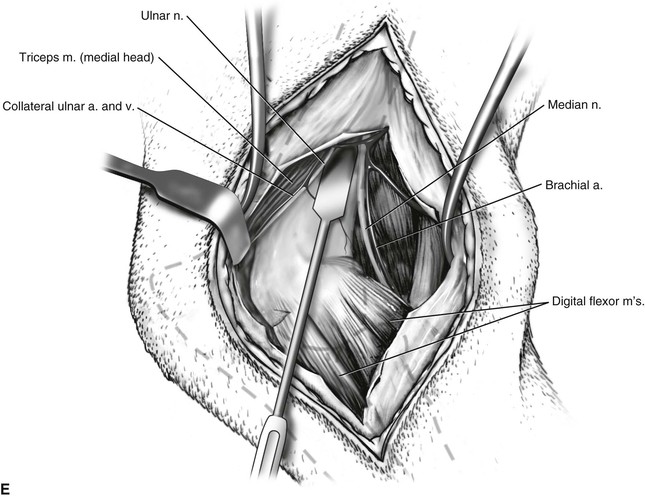
E In the cat, retraction of the neurovascular components is complicated by the passage of the brachial artery and median nerve through the supracondylar foramen of the humerus. Note also the short part of the medial head of the triceps brachii muscle running caudal to the medial aspect of the humeral condyle and inserting on the medial side of the olecranon process. If this muscle is elevated to expose a fracture line, care must be taken to protect the ulnar nerve deep to it.
Additional Exposure
Proximally, exposure of the medial side of the humerus is limited by the median nerve, which bifurcates from the ulnar nerve about the midshaft of the humerus and then courses craniodistally. Additional proximal exposure can be obtained by combining with the medial approach (see Plate 35), but these two approaches are not continuous. The brachial artery and vein and median and musculocutaneous nerves must be protected and carefully retracted (see Plate 35F).
Distally, exposure can be readily extended by combining with the approach to the medial humeral epicondyle (see Plate 48).
A separate approach to the lateral aspect of the humeral condyle and epicondyle (see Plate 39), in combination with this medial approach (see Plate 38), can be used for open reduction of supracondylar T-Y fractures of the distal humerus.
Approach to the Lateral Aspect of the Humeral Condyle and Epicondyle in the Dog
Based on a Procedure of Turner and Hohn49
Alternative Approaches
The approaches to the lateral (see Plate 40) and caudal (see Plate 42) humeroulnar parts of the elbow joint are alternatives, but exposure of the humeral articular surface for evaluation of intra-articular fracture reduction is very limited.
Description of the Procedure
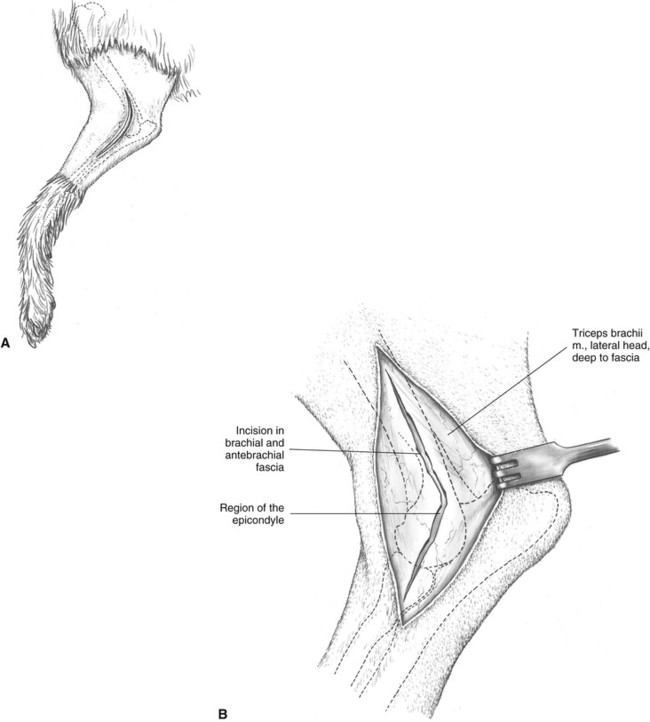
A Identify the lateral head of triceps muscle, lateral epicondyle, and olecranon by palpation. The skin incision extends along the lower fourth of the humerus and crosses the joint to end distally on the ulna. The incision passes over or slightly caudal to the lateral epicondyle. The subcutaneous fascia is incised on the same line.
B As the skin and subcutaneous fascia are retracted, the deep brachial and antebrachial fascia and the lateral head of the triceps muscle are exposed. An incision is made through the deep fascia along the cranial border of the triceps and is continued distally over the extensor muscles.
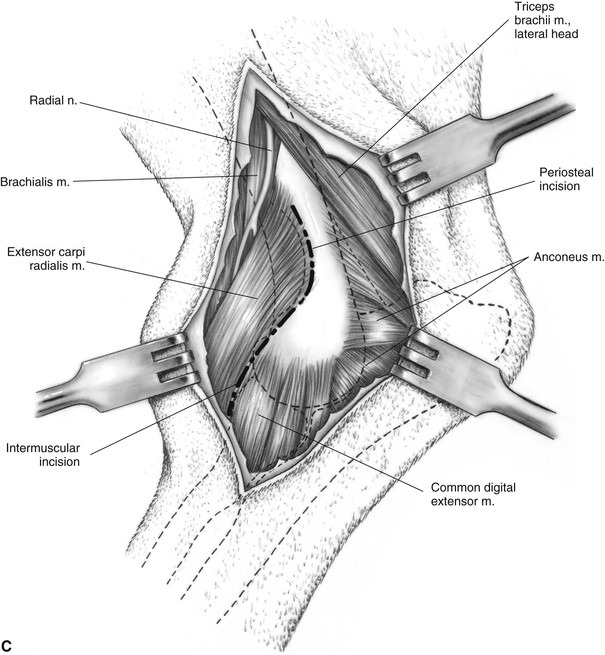
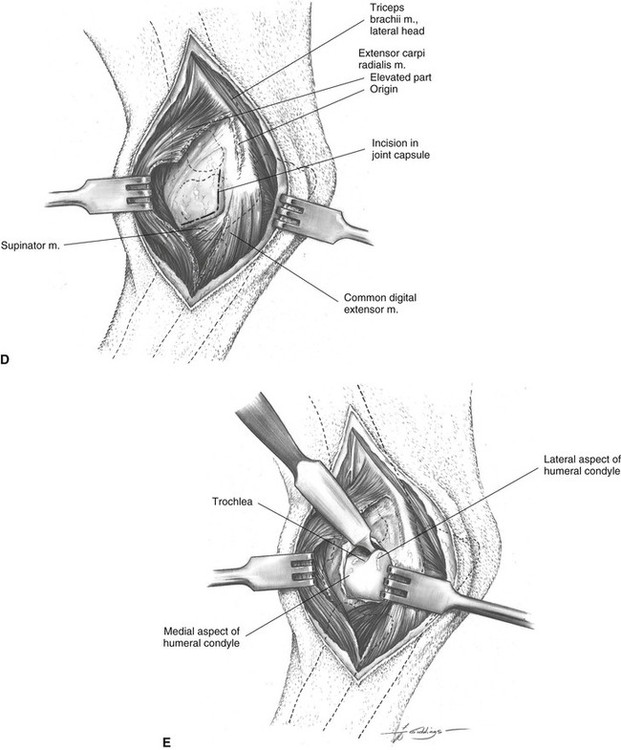
C Retraction of the fascia exposes the condylar region of the humerus. Although it is proximal to the main area of exposure, it is well to note the location of the radial nerve. An incision is started distally in the intermuscular septum between the extensor carpi radialis and the common digital extensor muscles. This incision continues proximally into the periosteal origin of the lateral half of the extensor carpi radialis muscle on the lateral epicondylar crest of the humerus.
D The extensor carpi radialis muscle is elevated from the bone and underlying joint capsule, and the capsule is opened with an L-shaped incision. Care must be taken to protect the articular cartilage of the condyle.
E Retraction of the joint capsule reveals the humeral condyle.
Additional Exposure
Additional proximal exposure is obtained in combination with the approach to the distal shaft of the humerus through a craniolateral incision (see Plate 37).
Additional distal exposure is obtained in combination with the approach to the head of the radius (see Plate 46) or the proximal metaphysis of the radius (see Plate 54).
This lateral approach (see Plate 39) can be used in combination with the medial approach to the distal shaft and supracondylar region of the humerus (see Plate 38) for open reduction of T-Y fractures of the distal humerus to avoid the need for olecranon osteotomy (see Plate 43) or triceps tenotomy (see Plate 44).
Precautions
Although not directly in the field, the radial nerve emerges from under the lateral head of the triceps muscle and runs obliquely craniodistal on the brachialis muscle. It bifurcates into superficial and deep branches that cross the flexor surface of the elbow medial to the origin of the extensor carpi radialis muscle.
Approach to the Lateral Aspect of the Humeral Condyle and Epicondyle in the Cat
Description of the Procedure
Although the steps in this approach for the cat are similar to those followed in the dog (Plate 39), the lateral head of the triceps muscle is relatively larger and overlies the lateral epicondyle of the humerus in the cat.
A Identify the lateral head of triceps muscle, lateral epicondyle, and olecranon by palpation. The skin incision extends along the lower fourth of the humerus and crosses the joint to end distally on the ulna. The incision passes over the lateral epicondyle. The subcutaneous fascia is incised on the same line.
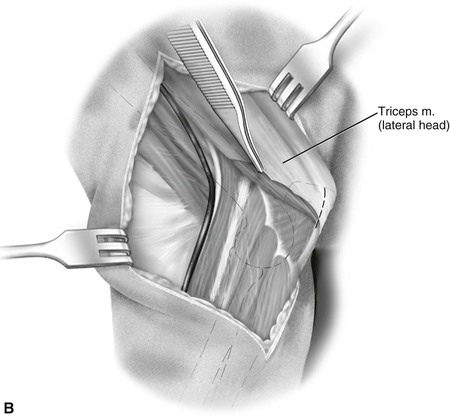
B As the skin and subcutaneous fascia are retracted, the deep brachial and antebrachial fascia and the lateral head of the triceps muscle are exposed. An incision is made through the deep fascia along the cranial border of the triceps and is continued distally over the extensor muscles. It may be necessary to partially transect some of the insertion of the lateral head of the triceps muscle on the lateral surface of the olecranon.
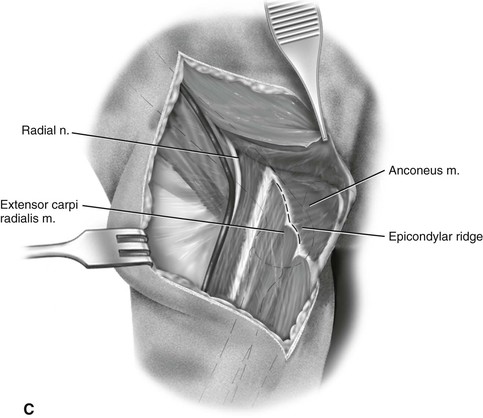
C Retraction of the lateral head of the triceps muscle exposes the condylar region of the humerus. Although it is proximal to the main area of exposure, it is well to note the location of the radial nerve. An incision is started distally in the intermuscular septum between the extensor carpi radialis and the common digital extensor muscles. This incision continues proximally into the periosteal origin of the extensor carpi radialis muscle on the lateral epicondylar crest of the humerus.
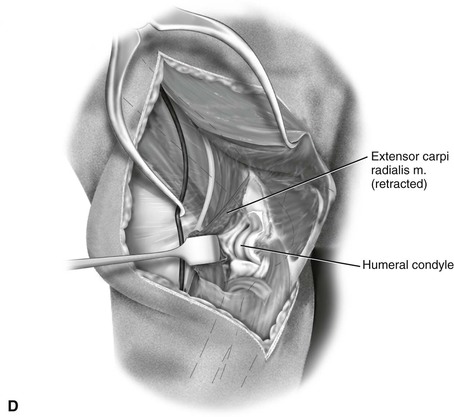
D The extensor carpi radialis muscle is elevated from the bone and underlying joint capsule, and the capsule is opened with an L-shaped incision. Care must be taken to protect the articular cartilage of the condyle. Retraction of the joint capsule reveals the humeral condyle.
Precautions
Although not directly in the field, the radial nerve emerges from under the lateral head of the triceps muscle and runs obliquely craniodistal on the brachialis muscle. It bifurcates into superficial and deep branches that cross the flexor surface of the elbow medial to the origin of the extensor carpi radialis muscle.

Approach to the Lateral Humeroulnar Part of the Elbow Joint
Based on a Procedure of Snavely and Hohn46
Alternative Approaches
Alternative approaches through a lateral incision provide exposure of the lateral aspect of the condyle and epicondyle (see Plate 39) and the caudal humeroulnar joint compartment (see Plate 42).
Description of the Procedure
A The skin incision is centered on the lateral humeral epicondyle, which is easily palpated. The incision curves to follow the lateral epicondylar crest and the proximal radius.
B Subcutaneous fascia is incised on the same line as the skin. The fascia of the brachium is incised along the cranial border of the lateral head of the triceps brachii to its insertion on the olecranon.
C Elevation of the triceps brachii exposes the anconeus muscle, which is incised at its periosteal origin on the lateral epicondylar crest.
D Subperiosteal elevation of the origin of the anconeus muscle exposes the caudolateral compartment of the elbow and the anconeal process of the ulna.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


