The Pelvis and Hip Joint
 . Approach to the Wing of the Ilium and Dorsal Aspect of the Sacrum
. Approach to the Wing of the Ilium and Dorsal Aspect of the Sacrum
 . Approach to the Ilium Through a Lateral Incision
. Approach to the Ilium Through a Lateral Incision
 . Approach to the Ventral Aspect of the Sacrum
. Approach to the Ventral Aspect of the Sacrum
 . Approach to the Craniodorsal Aspect of the Hip Joint Through a Craniolateral Incision in the Dog
. Approach to the Craniodorsal Aspect of the Hip Joint Through a Craniolateral Incision in the Dog
 . Approach to the Craniodorsal Aspect of the Hip Joint Through a Craniolateral Incision in the Cat
. Approach to the Craniodorsal Aspect of the Hip Joint Through a Craniolateral Incision in the Cat
 . Approach to the Dorsal Aspect of the Hip Joint Through an Intergluteal Incision
. Approach to the Dorsal Aspect of the Hip Joint Through an Intergluteal Incision
 . Approach to the Craniodorsal and Caudodorsal Aspects of the Hip Joint by Osteotomy of the Greater Trochanter
. Approach to the Craniodorsal and Caudodorsal Aspects of the Hip Joint by Osteotomy of the Greater Trochanter
 . Approach to the Craniodorsal and Caudodorsal Aspects of the Hip Joint by Tenotomy of the Gluteal Muscles
. Approach to the Craniodorsal and Caudodorsal Aspects of the Hip Joint by Tenotomy of the Gluteal Muscles
 . Approach to the Caudal Aspect of the Hip Joint and Body of the Ischium
. Approach to the Caudal Aspect of the Hip Joint and Body of the Ischium
 . Approach to the Lateral Aspect of the Hemipelvis
. Approach to the Lateral Aspect of the Hemipelvis
 . Approach to the Ventral Aspect of the Hip Joint or the Ramus of the Pubis
. Approach to the Ventral Aspect of the Hip Joint or the Ramus of the Pubis
 . Approach to the Pubis and Pelvic Symphysis
. Approach to the Pubis and Pelvic Symphysis
 . Approach to the Ischium
. Approach to the IschiumApproach to the Wing of the Ilium and Dorsal Aspect of the Sacrum
Based on a Procedure of Alexander, Archibald, and Cawley2
Alternative Approaches
Dorsal midline exposure of fractures and luxations of lumbar vertebra 7 and the sacrum is obtained via the dorsal approach (see Plate 21).
To gain exposure of both the wing and shaft of the ilium, use the “gluteal roll-up” approach through a lateral incision (see Plate 64).
The ventral approach is an alternative means of gaining exposure of the sacroiliac joint (see Plate 65). An advantage of the ventral approach is that it can readily be combined with the lateral approach to the ilial shaft (see Plate 64).
Description of the Procedure
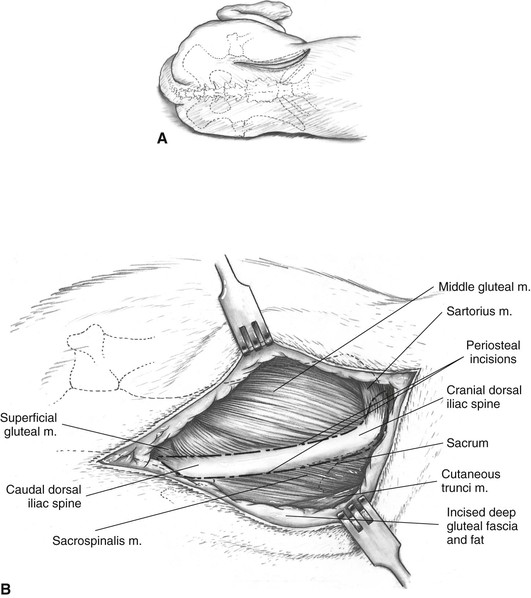
A The skin incision starts cranially over the cranial dorsal iliac spine and continues caudally parallel to the midline to near the hip joint. Subcutaneous tissues and gluteal fascia and fat are incised on the same line to expose the cranial and caudal dorsal iliac spines.
B If only the lateral (gluteal) surface of the wing of the ilium needs to be exposed, as for fractures or cancellous bone collection, an incision is made in the periosteal origin of the middle gluteal muscle on the lateral edge of the ilium near the cranial dorsal iliac spine and ending beyond the caudal dorsal spine. If the sacrum must also be exposed, a second incision is made in the periosteal origin of the sacrospinalis muscle, at the medial edge of the ilium. These incisions merge as they continue caudally, and it will be necessary to transect some fibers of the superficial gluteal muscle in this region.
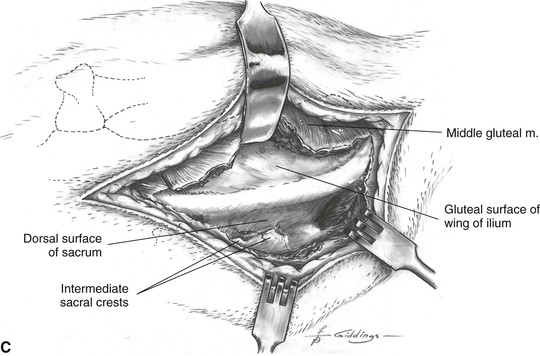
C The middle gluteal muscle is elevated subperiosteally in young animals, or simply scraped from its origin on the ilium in older animals. The elevation continues caudally to the caudal dorsal iliac spine. Continuing further, caudal dissection will result in severance of the cranial gluteal artery, vein, and nerve. Similar elevation of the sacrospinalis muscle on the medial side of the ilium gives limited exposure of the dorsal surface of the sacrum. Muscular elevation on the sacrum should be confined to the area lateral to the intermediate crests to avoid damage to dorsal nerve roots emerging through the dorsal foramina of the sacrum.
Precautions
The approach should not be extended caudally beyond the caudal dorsal iliac spine. The cranial gluteal nerve arises as a branch of the lumbosacral trunk, just caudoventral to the sacroiliac joint. Accompanied by the cranial gluteal artery and vein, it then circles dorsally across the shaft of the ilium at the origin of the caudal bundle of the deep gluteal muscle.
Approach to the Ilium Through a Lateral Incision
Based on a Procedure of Hohn and Janes22
Alternative Approach
The dorsal approach (see Plate 63) can be used if exposure of only the iliac wing is needed.
Description of the Procedure
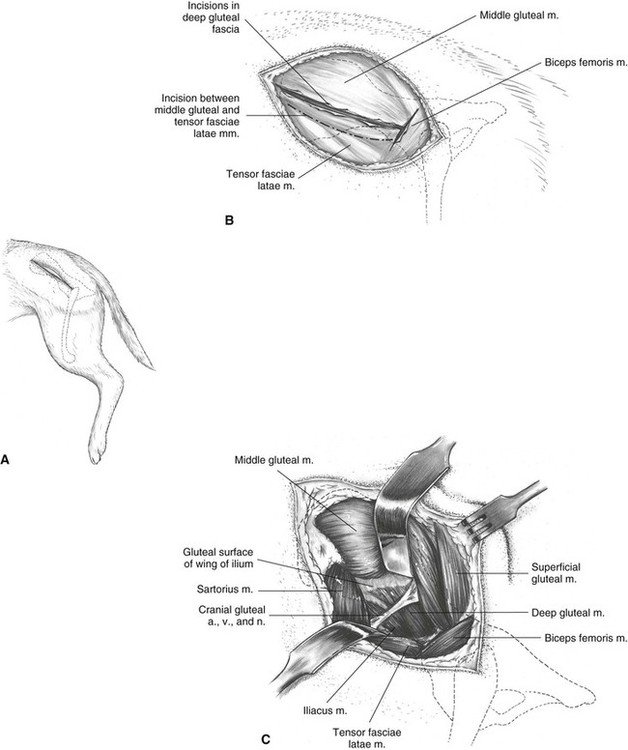
A The skin incision extends from the center of the iliac crest and ends just caudal and distal to the greater trochanter.
B Subcutaneous tissues, gluteal fat, and superficial fascia are incised and elevated with the skin. Incision of the deep gluteal fascia on the same line as the skin allows incision of the intermuscular septum between the tensor fasciae latae and middle gluteal muscles. This incision extends from the ventral iliac spine to the cranial border of the biceps femoris muscle. Fascia is also incised along the cranial border of the biceps femoris muscle to create a T-shaped fascial incision.
C Retraction of the middle gluteal muscle exposes the deep gluteal muscle and a portion of the iliac shaft.
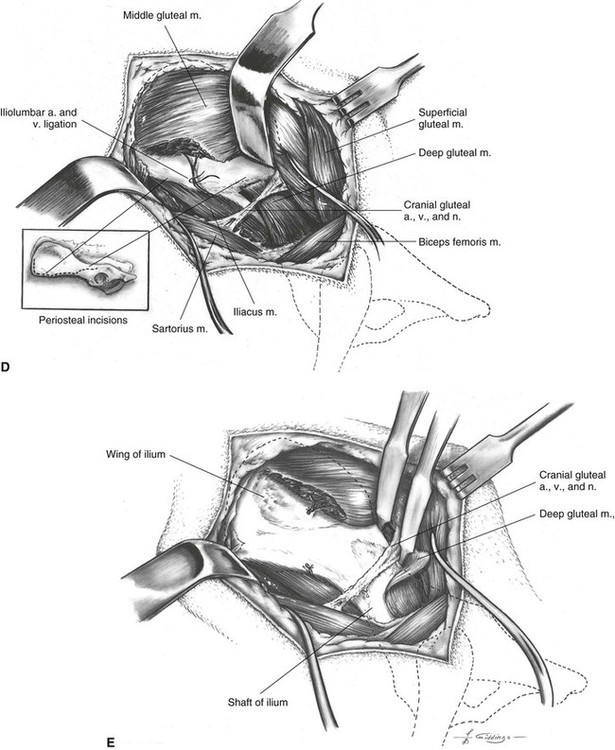
D An incision is made in the origin of the middle gluteal muscle on the ilium, starting at the caudal ventral iliac spine and continuing cranially and dorsally as needed. Some sharp dissection may be needed between the middle gluteal and sartorius muscles, the fibers of which blend together. The iliolumbar vessels are ligated at the ventral edge of the ilium. An incision is started in the origin of the deep gluteal muscle to allow caudal retraction of this muscle.
E Subperiosteal elevation of the gluteal muscles exposes the crest, wing, and shaft of the ilium.
Maximal exposure of the shaft of the ilium, cranial to the acetabulum, may necessitate sacrificing branches of the cranial gluteal artery, vein, and nerve that supply the tensor fasciae latae muscle. Elevation of the iliacus muscle along the ventral border of the iliac shaft (see Plate 65) usually results in severing a nutrient artery on the ventral aspect of the shaft. The severed artery must then be cauterized or plugged with bone wax.
Additional Exposure
Extension of this approach cranioventrally provides exposure of the ventral aspect of the sacrum and sacroiliac joint (see Plate 65).
Additional exposure of the cranial margin of the acetabulum and femoral head and neck is obtained in combination with the craniolateral exposure of the hip joint (see Plate 66).
For exposure of both the ilial shaft and dorsal rim of the acetabulum, this lateral approach can be combined with the dorsal approaches to the hip joint by osteotomy of the greater trochanter (see Plate 69) or gluteal tenotomy (see Plate 70).
Precautions
Consideration must be given to the sciatic nerve when retracting the gluteal muscles (see Plate 64E) or using bone-holding forceps on the ilium. The nerve lies close to the dorsomedial aspect of the iliac shaft. With care in retracting, the cranial gluteal vessels and nerve can usually be preserved.
Approach to the Ventral Aspect of the Sacrum
Based on a Procedure of Montavon, Boudrieau, and Hohn27
Alternative Approach
The approach to the sacroiliac joint through a dorsal incision (see Plate 63) allows superior visualization of the sacral wing in sacroiliac luxation. However, a disadvantage of the dorsal approach is that it cannot be extended caudally for a combined exposure of the ilial shaft and hip joint.
Description of the Procedure
This approach is an extension of Approach to the Ilium Through a Lateral Incision and should be performed as shown in Plate 64A-C. Elevation of the deep gluteal muscle, as shown in Plate 64D and E, is unnecessary.
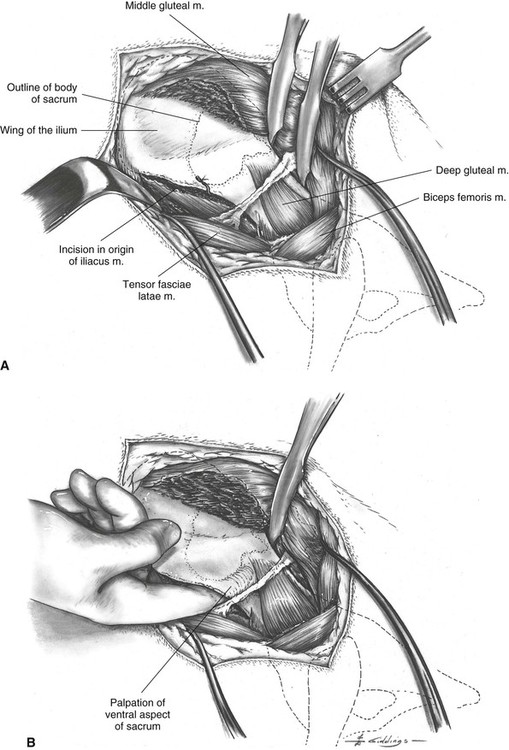
A The iliacus muscle is incised at its origin along the ventromedial border of the ilium and is subperiosteally elevated sufficiently to allow insertion of a finger into the pelvic canal. The nutrient artery of the ilium may be disrupted during elevation of the iliacus muscle and is best controlled by cautery or bone wax.
B The body of the sacrum is palpable now; in the case of a sacroiliac luxation, the whole ilial body and wing are mobile enough that the region of the synchondrosis can be palpated on the medial side of the ilium, and the smooth articular surface can be felt on the sacral wing.
Additional Exposure
Complete exposure of the sacroiliac joint and ilial shaft is obtained by combining this approach with the lateral approach (see Plate 64).
By extending the muscle elevation craniodorsally around the iliac crest, the approach can be combined with the approach to the wing of the ilium and dorsal aspect of the sacrum (see Plate 63). This allows direct visualization of the sacroiliac joint, which is useful when fractures are present. However, this combined approach may result in significant disruption of the origin of the middle gluteal muscle.
Precautions
The lumbosacral trunk, arising from the ventral branches of the sixth and seventh lumbar nerves and the first sacral nerve, originates ventral to the sacroiliac joint. It passes medial to the ilial shaft and at the greater ischiatic foramen receives a branch from the second sacral nerve, at which point it becomes the sciatic nerve.
Approach to the Craniodorsal Aspect of the Hip Joint Through a Craniolateral Incision in the Dog
Based on Procedures of Archibald, Brown, Nasti, and Medway3 and Brown and Rosen6
Alternative Approaches
Greater exposure of the hip joint and dorsum of the acetabulum is provided by the dorsal approach with osteotomy of the greater trochanter (see Plate 69) or with gluteal tenotomy (see Plate 70).
The approach to the ventral aspect of the hip joint (see Plate 73) is an alternative for femoral head and neck resection, but the amount of exposure gained is very limited.
The approach to the caudal aspect of the hip joint is an alternative for open reduction of craniodorsal coxofemoral luxation (see Plate 71).
Description of the Procedure
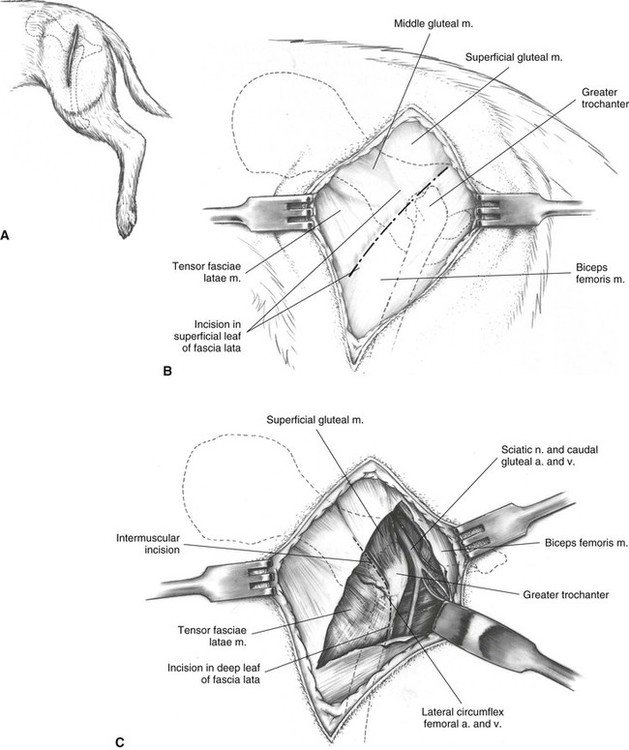
A The skin incision is centered at the level of the greater trochanter and lies over the cranial border of the shaft of the femur. Distally, it extends one third to one half the length of the femur; proximally, it curves slightly cranially to end just short of the dorsal midline. When performing the total hip replacement procedure, the skin incision is modified to facilitate femoral reaming; proximally it curves caudally over the trochanter and toward the base of the tail.
B The skin margins are undermined and retracted. An incision is made through the superficial leaf of the fascia lata, along the cranial border of the biceps femoris muscle.
C The biceps femoris muscle is retracted caudally to allow incision in the deep leaf of the fascia lata to free the insertion of the tensor fasciae latae muscle. The incision continues proximally through the intermuscular septum between the cranial border of the superficial gluteal muscle and the tensor fasciae latae muscle.
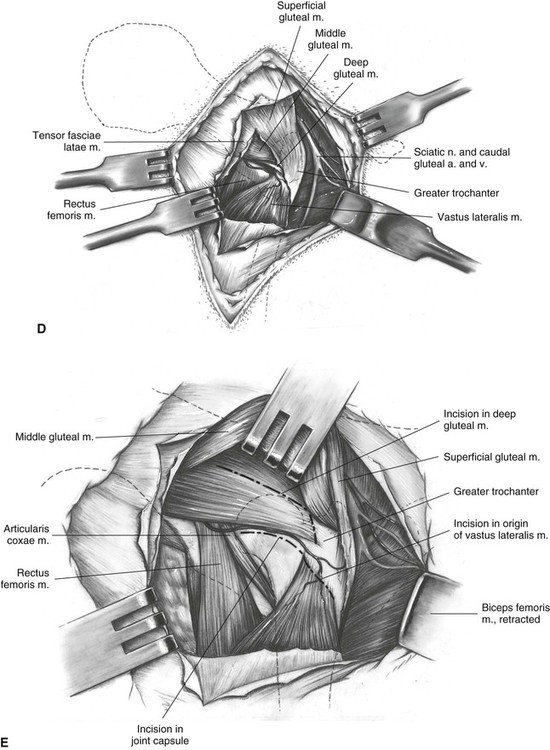
D The fascia lata and the attached tensor fasciae latae muscle are retracted cranially and the biceps caudally. Blunt dissection and separation along the neck of the femur with the fingertip allows visualization of a triangle bounded dorsally by the middle and deep gluteal muscles, laterally by the vastus lateralis muscle, and medially by the rectus femoris muscle.
E The joint capsule is covered by areolar tissue, which must be cleared away by blunt dissection. An incision is then made in the joint capsule and continued laterally along the femoral neck through the origin of the vastus lateralis muscle on the neck and lesser trochanter. Exposure can be improved by tenotomy of a portion of the deep gluteal tendon close to the trochanter, leaving enough tendon on the bone to allow suturing. The muscle is split proximally, parallel to its fibers, and the pedicle is allowed to retract.
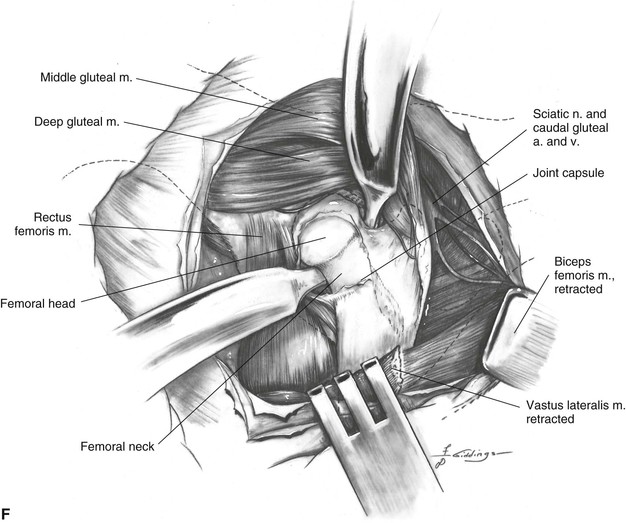
F The origin of the vastus lateralis muscle is elevated from the femoral neck and reflected distally. The muscle comes free most easily if the elevation proceeds from distal to proximal. This elevation can be subperiosteal in the immature animal or extraperiosteal in the mature animal. Hohmann retractors are placed intracapsularly ventral and caudal to the femoral neck to allow visualization of the femoral head. Caution is needed to be certain that the caudal retractor is intracapsular, or at least between the deep gluteal muscle and the femoral neck, to avoid entrapping the sciatic nerve on the caudodorsal surface of the deep gluteal muscle.
Additional Exposure
Extension of this approach cranially to gain exposure of the ilial shaft is possible by combining with the approach to the ilium through a lateral incision (see Plate 64).
Distally, exposure of the femur can be obtained in combination with the approach to the greater trochanter and subtrochanteric region of the femur (see Plate 76) or the approach to the shaft of the femur (see Plate 77).
Closure
One or two mattress sutures (see Figure 21B) or a pulley suture (see Figure 21D) are placed in the deep gluteal tendon incision, and the origin of the vastus lateralis muscle is sutured to the cranial edge of the deep gluteal muscle. Continuous sutures are placed in the insertion of the tensor fasciae latae muscle distally and are continued proximally along the cranial border of the superficial gluteal muscle. The superficial leaf of the fascia lata distally and the gluteal fascia proximally are closed to the cranial border of the biceps femoris with a continuous pattern. The rest of the incision is closed routinely in layers.
Precautions
Dorsal to the hip joint, the sciatic nerve emerges from the ischiatic foramen under the superficial gluteal muscle. It passes caudal to the deep gluteal muscle, across the gemelli and internal obturator muscles, then passes down the thigh deep to the biceps femoris muscle. To reduce the risk of damage to the sciatic nerve, sharp retractors such as the Meyerding should not be used to retract the biceps femoris muscle.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


