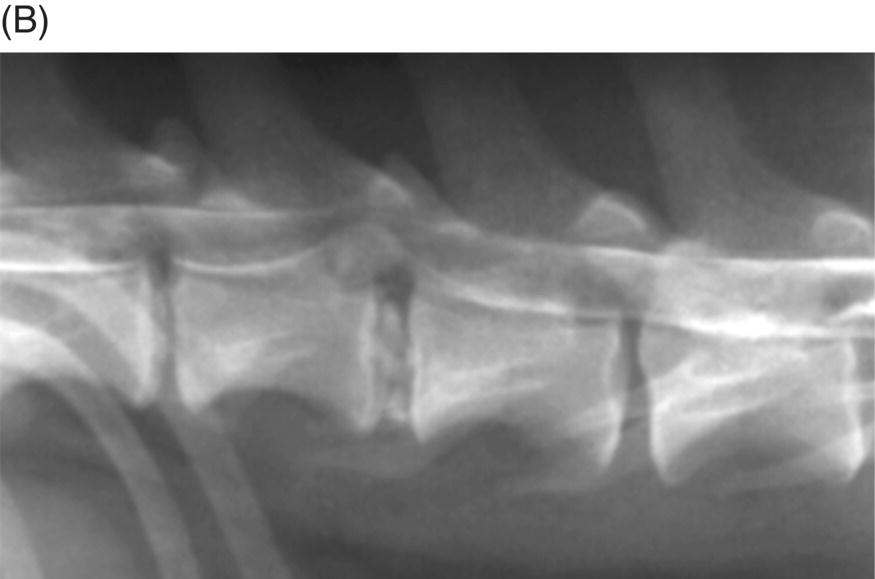
28 James M. Fingeroth When patients are referred for surgical treatment of suspected intervertebral disc (IVD) disease, there are some assumptions made that may not always be applicable in every case, or which can mislead both the referring veterinarian and the surgeon. It has already been established elsewhere in this text that clinical signs may be suggestive of an intervertebral disc etiology; however, in the absence of definitive imaging studies that correlate with the neurologic examination, it remains only a speculation that IVD disease (IVDD) is the underlying problem. Moreover, it has been demonstrated throughout the text that one must be careful to distinguish IVD disease (wherein we may find evidence based on signalment, the neurologic exam, or plain radiographic findings) from actual disc herniation (Figure 28.1). It is only for the latter cases that surgery is felt to have a therapeutic role. Furthermore, it has been demonstrated elsewhere in the text that not all disc herniations result in lingering compression of the spinal cord or nerve roots. This is critically important, since the main thrust of surgery for disc disease is predicated on the concept of decompression (Figure 28.2). The issue of concussive versus compressive spinal cord injury is addressed in Chapter 15, and it is on that basis that we utilize surgery to treat the latter in hopes of more rapidly reversing the effects of spinal cord injury and preventing further parenchymal changes that could lead to permanent paralysis. Figure 28.1 (A) Lateral radiograph of the cervical spine of a dog with signs of a cervical myelopathy. Note the mineralized intervertebral disc at C6–C7 (arrow). This is clearly an example of intervertebral disc disease (IVDD). However, note also the collapsed disc space at C2–C3. This too represents radiographic evidence of IVDD. Subsequent imaging confirmed that spinal cord compression was occurring from disc herniation at the C2–C3 level. One has to be careful to avoid seeing evidence of IVDD on plain radiographs and concluding that clinical signs are due to that lesion. In particular, the presence of mineralization confined to within the disc space only indicates IVDD and not necessarily IVDH. (B) In this instance from a lumbar spine, there is mineralized disc material both in the disc space and within the vertebral canal, and the myelogram confirms that this is herniated disc material causing spinal cord compression.
What Constitutes Spinal Cord Decompression?

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


