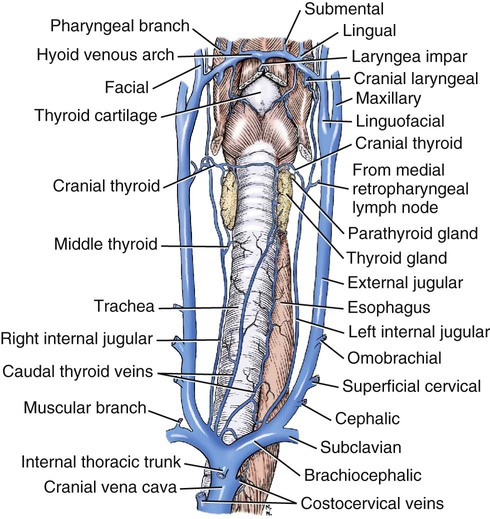
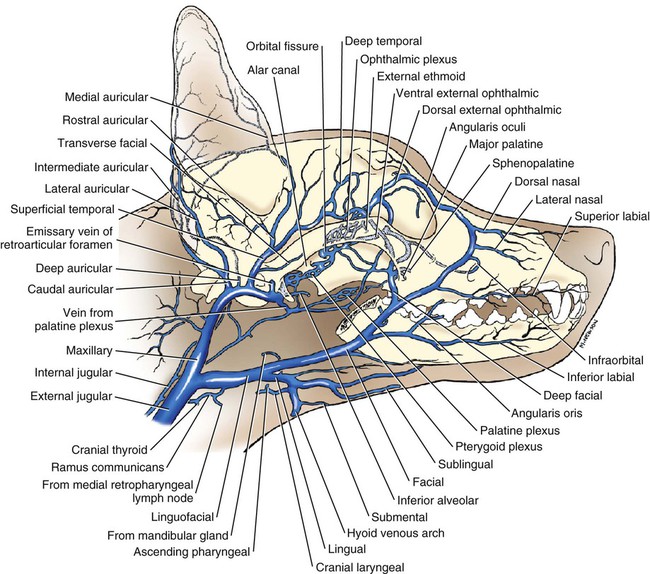
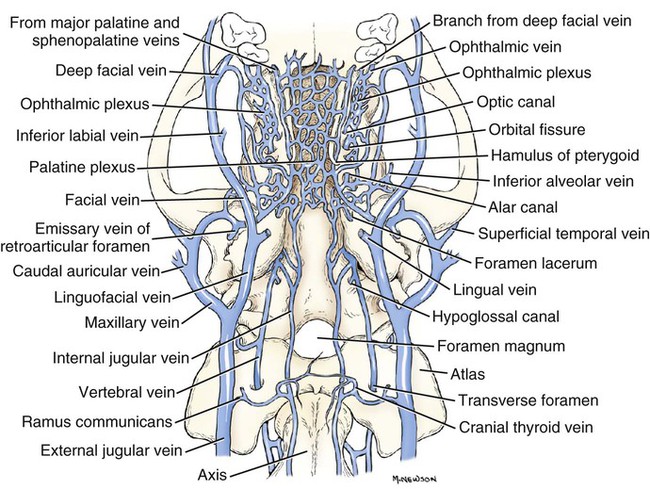
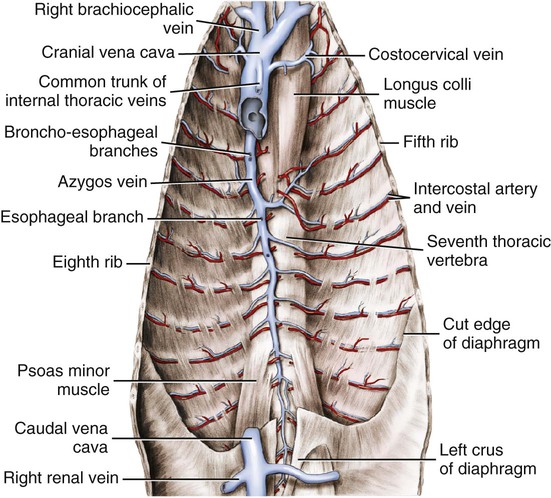
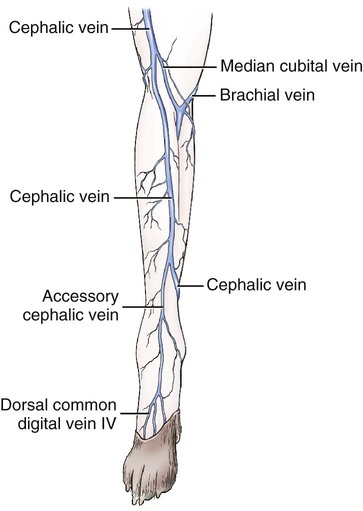
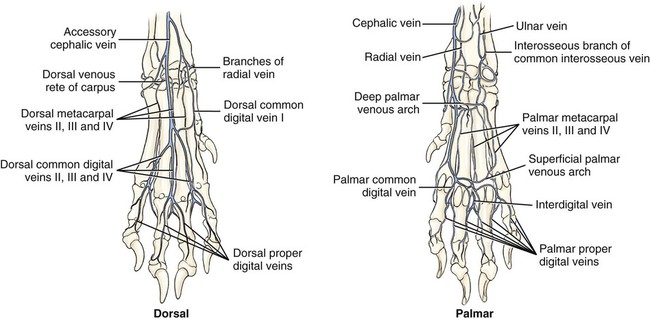
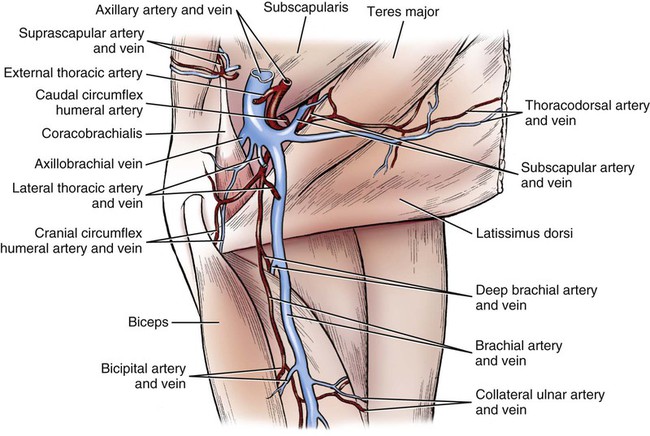
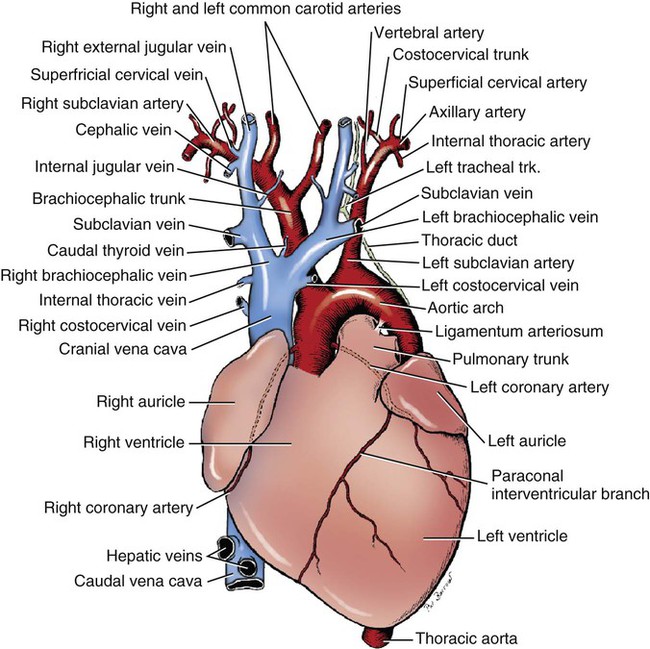
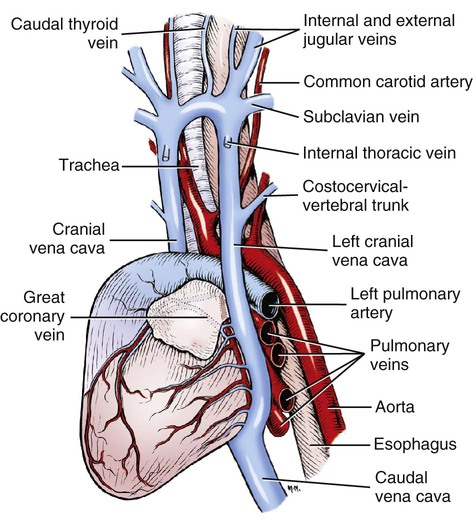
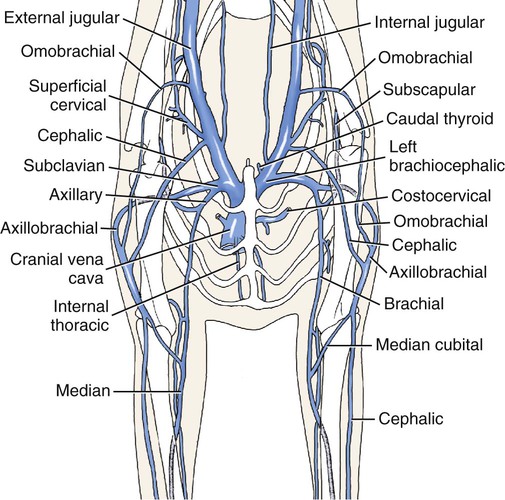
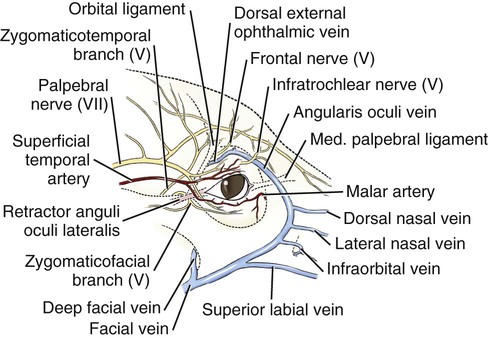
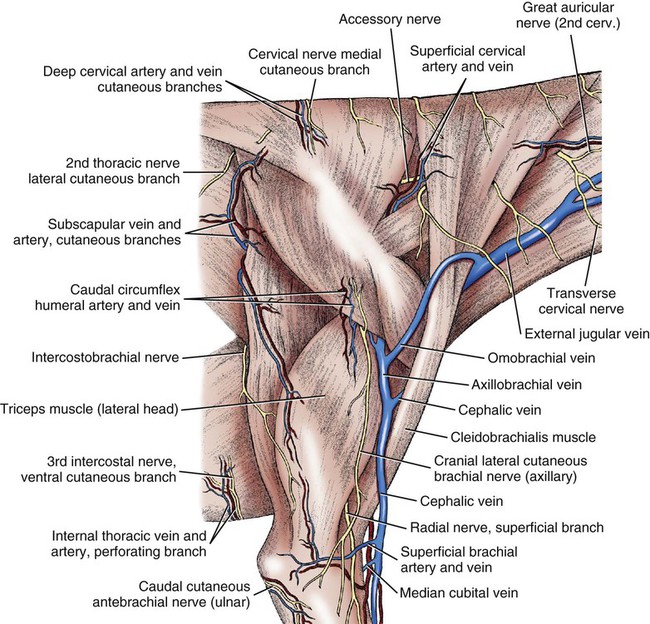
Veins follow the same general course as arteries, although variations in their number, size, and course are more frequent than in arteries. The accompanying veins are known as satellite veins, or venae comitantes, and often take the same name as the artery they accompany (Fig. 12-1). Although the smaller satellite veins are frequently double, the larger veins are single, as are most of the deep veins. All systemic veins have thin walls, and most have a large lumen in comparison with the arteries. The pressure in the veins is low, and the blood flows much more slowly in them than in the arteries. Stone and Stewart (1988) discussed the architecture and structure of canine veins, with special reference to confluences. Because there is generally no pulse in the venous system, the movement of blood depends primarily on pressure relations in the thorax and on muscular activity. The contraction of muscles results in compression of the veins, thus propelling the contained blood toward the heart. Negative pressure in the thorax during inspiration and the presence in most veins of semilunar valves that prevent backflow augment this effect of the skeletal and visceral muscles. Veins farthest from the heart contain the most valves. For an overview, see Shepherd and Vanhoutte (1975) as well as the older classic work by Franklin (1937). Simoens et al. (1984) have illustrated, characterized, and referenced the 963 veins of domestic animals (including the dog) that were listed in the 1973 edition of Nomina Anatomica Veterinaria. Cardiac and pulmonary veins are discussed with the heart in Chapter 11. The cranial vena cava (v. cava cranialis), formerly called precava (Figs. 12-1 through 12-5), is an unpaired vessel, 1.5 to 2 cm in diameter and 8 to 12 cm long. It lies in the cranial mediastinum ventral to the trachea and is in contact with the esophagus on its left side. It is also in contact with the thymus when this gland is fully developed. It runs through the cranial mediastinum and is the most ventral of the several structures that course through the thoracic inlet. It is formed, at a level just cranial to the thoracic inlet, by the convergence of the right and left brachiocephalic veins. These form an angle, open cranially, of approximately 90 degrees, so that each vein enters the cranial vena cava at an angle of approximately 45 degrees with the median plane. The cranial vena cava empties into the cranial part of the right atrium. Some mammals, such as the rabbit, retain the embryonic pattern of paired cranial venae cavae draining into the sinus venarum of the right atrium. As would be expected, this condition (see Fig. 12-3) is often seen as an anomaly in other animals, including the dog (Fig. 12-3). Cox et al. (1991) describe an example in a horse and make reference to reports in the dog. Sekeles (1982), in his case report for a cow, referred to literature citing 21 reported instances of persistent left venae cavae in the dog. For other reports of this anomaly in the dog see Stoland and Latimer (1947), Schaller (1955), Buchanan (1963), Gomercič (1967), Hutton (1969), Buergelt and Wheaton (1970), and Larcher et al. (2006). The costocervical vein (v. costocervicalis) (Figs. 12-2 and 12-4) is medial to the proximal end of the first rib. The left vein runs lateral to the left subclavian artery and empties into the dorsolateral surface of the cranial part of the cranial vena cava. It may terminate in the left brachiocephalic vein. The right costocervical vein, approximately 1 cm caudal to the left at its termination, crosses the lateral surface of the trachea and enters the cranial vena cava ventral to the brachiocephalic trunk and vagus nerve. The right costocervical vein is approximately 3 cm long; that of the left side is approximately 4 cm. Both vessels are approximately 5 mm in diameter. Intervertebral veins (vv. intervertebrales) (Figs. 12-26 through 12-28) pass through the intervertebral foramen and connect the ventral internal vertebral venous plexus with the ventral external vertebral venous plexus. The last or eighth cervical intervertebral vein regularly bifurcates into a cranial communicating vein that joins the vertebral vein and a caudal communicating vein that empties into the deep cervical vein. According to Worthman (1956), the supreme intercostal vein receives the second and third thoracic intervertebral veins on each side. In almost half of his specimens, the fourth thoracic intervertebral vein on the left also emptied into the supreme intercostal vein of the same side. The vertebral vein (v. vertebralis) (Figs. 12-1, 12-8, 12-22, 12-23, and 12-26) begins by the confluence of the emissary vein of the hypoglossal canal, if present, and the sigmoid sinus and ventral petrosal sinus in the space between the jugular foramen and the tympanooccipital fissure. The small internal jugular vein also arises wholly or partly at this confluence. The vertebral vein is approximately 1.5 mm in diameter as it runs caudally across the ventrolateral part of the atlantooccipital joint, then ventral to the wing of the atlas to the transverse foramen. It receives the first intervertebral vein, which leaves the ventral internal vertebral venous plexus, passes through the lateral vertebral foramen of the atlas and then through the alar notch, and joins the vertebral vein in the atlantal fossa. Worthman (1956) and Dräger (1937) call the initial portion of the vertebral vein the occipital vein, although only a segment of it parallels the occipital artery. The dog, however, may be regarded as not having a true occipital vein (v. occipitalis), because the dorsal nuchal area supplied by the occipital artery is drained by the occipital emissary vein and the ventral portion supplied by the occipital artery is drained by the vertebral vein. The internal thoracic vein (v. thoracica interna) (Figs. 12-1 through 12-4) is unpaired at its termination in the middle of the ventral surface of the cranial vena cava in approximately half of all specimens. In such instances it usually ranges from 1 to 4 cm in length. In the specimens in which it is paired, the right vein usually enters the cranial vena cava, whereas the left enters the left brachiocephalic vein. The peripheral part of the internal thoracic vein and its branches are prominent satellites of the comparable parts of the internal thoracic artery. Tributaries of the internal thoracic vein parallel the arteries and include pericardiacophrenic, thymic, mediastinal, ventral intercostal, perforating, and musculophrenic veins. The cranial epigastric vein of the abdomen is an extension of the internal thoracic vein. The brachiocephalic vein (v. brachiocephalica) (Figs. 12-2, 12-4, and 12-5) merges with its fellow of the opposite side cranial to the thoracic inlet to form the cranial vena cava. Each is approximately 1 cm in diameter, and is formed by the joining of the caudally coursing external jugular and the medially coursing subclavian vein. Unlike the comparable artery, no part of the venous channel coming from the thoracic limb normally lies within the thorax. There is therefore no basis for naming a portion of the channel for venous return from the thoracic limb the subclavian vein. The subclavian vein has no tributaries and only consists of the very short vein connecting the axillary vein at the first rib to the external jugular vein to form the brachiocephalic vein. The merging brachiocephalic veins lie ventral to the trachea and esophagus as the most ventral structures in this region. The left brachiocephalic vein is longer than the right as it must cross the median plane to reach the right brachiocephalic vein to form cranial vena cava on the right. The caudal thyroid vein and the internal jugular veins enter the brachiocephalic as well as the left costocervical vein in some dogs. The caudal thyroid vein (v. thyroidea caudalis) (Figs. 12-2 through 12-5) is an unpaired vein, approximately 1 mm in diameter, which arises primarily from the deep surfaces of the sternothyrohyoid muscles, but on one or both sides its most cranial tributary may arise in the thyroid lobe or lobes. It terminates usually in the cranial angle formed by the merging brachiocephalic veins. This was formerly known as the v. thyroidea ima. The internal jugular vein (v. jugularis interna) (Figs. 12-3 through 12-6, 12-8, 12-22, and 12-23), approximately 1 mm in diameter, is formed in the tympanooccipital fissure by the confluence of the ventral petrosal and sigmoid sinuses, and, occasionally, the vein of the hypoglossal canal. Its initial portion may be double. The internal jugular vein lies at first in association with the internal carotid artery and then in the sheath of the common carotid artery. In the vicinity of the larynx, it receives an anastomotic branch from the laryngeal or pharyngeal tributary of the lingual vein. Caudal to the larynx it receives the cranial thyroid vein (v. thyroidea cranialis) from the cranial pole of the thyroid lobe. Opposite this tributary there is occasionally a second anastomotic connection with the external jugular vein. A branch from the medial retropharyngeal lymph node is also received here. Frequently, it receives the small middle thyroid vein (v. thyroidea media), which comes from the caudal pole of one or both thyroid lobes. On either or both sides, this vein may terminate in the brachiocephalic vein rather than the internal jugular vein, in which case it is considered to be the caudal thyroid vein. The internal jugular vein usually terminates in the caudal portion of the external jugular vein; rarely it terminates in the brachiocephalic vein. The external jugular vein (v. jugularis externa) (Figs. 12-1 though 12-6, 12-8, and 12-10) is the main channel for return of venous blood from the head. It begins by the union of the linguofacial and maxillary veins, caudal to the mandibular salivary gland or at a transverse plane through the cricoid cartilage and the axis. It is approximately 1 cm in diameter and 12 cm long. In the adult it contains a few nonfunctional valves, which are irregular in their spacing. As the external jugular vein runs caudally in the superficial fascia, it crosses the lateral surface of the cleidocephalic muscle obliquely. The external jugular vein lies directly deep to the skin and is commonly used for venipuncture in dogs that are too small for the procedure to be feasible in the smaller veins of the extremities. At the cranial border of the shoulder, it receives the omobrachial and cephalic veins that course proximally from the brachium. Approximately 2 cm caudal to the termination of the omobrachial vein, the external jugular receives the superficial cervical vein (v. cervicalis superficialis), but this is variable. At its termination, the external jugular vein usually receives the internal jugular vein on its medial side. The linguofacial vein (v. linguofacialis) (Figs. 12-1, 12-5, 12-6, and 12-8) begins by the confluence of the lingual and facial veins ventral to the mandibular salivary gland. It may have one or more tributaries from the capsule of the mandibular gland, and regularly receives the glandular vein (v. glandularis), which leaves the caudal pole of the gland. It contains a valve at its termination. The facial vein (v. facialis) (Figs. 12-6 and 12-7) begins on the dorsolateral surface of the muzzle, covered by the m. levator nasolabialis. It is formed by the confluence of the smaller dorsal nasal vein (v. nasalis dorsalis), which drains the dorsolateral surface of the nose, and the larger angular vein of the eye. The dorsal external ophthalmic vein (v. ophthalmica externa dorsalis) (Figs. 12-6, 12-7, and 12-22) runs approximately 2 cm caudally into the orbit and forms the ophthalmic plexus (plexus ophthalmicus) (see Figs. 12-6 and 12-22). The plexus lies within the periorbita. It extends to the orbital fissure, and therefore lies in the caudal two thirds of the orbit. The plexus becomes consolidated at the orbital fissure and, after traversing it, joins the cavernous sinus. Dorsally, a small branch runs through the optic canal to join its fellow and the dorsal petrosal sinus of its side (Fig. 12-24). Ventrally, the plexus is continued caudally outside the alar canal and is to be regarded as the beginning of the maxillary vein. A second connection between the ophthalmic system and the maxillary vein exists here in the form of a vein that runs through the alar canal. This vein also communicates with the cavernous sinus by an emissary vein that traverses the round foramen (v. emissaria foraminis rotundi). The ventral external ophthalmic vein (v. ophthalmica externa ventralis) (see Fig. 12-6) joins the dorsal external ophthalmic vein as well as the ophthalmic plexus caudally. Caudal to the eyeball an anastomotic branch unites the dorsal and ventral external ophthalmic veins. At the eyeball, the ventral external ophthalmic vein turns ventrally, receives the ventral vorticose veins and a branch from the third eyelid before anastomosing with the deep facial vein. Two emissary veins join the ophthalmic plexus. One of these is the external ethmoidal vein (v. ethmoidalis externa) (see Fig. 12-6), a satellite of the like-named artery, which passes through the ethmoidal foramen. The other emissary vein is the frontal diploic vein (v. diploica frontalis), from the diploë of the frontal bone, which passes through a small supraorbital foramen in the zygomatic process of the frontal bone. The latter vein may join the dorsal external ophthalmic vein before the plexus is formed. The nasal venous vascular bed has been investigated by Lung and Wang (1989). The lateral nasal vein (v. lateralis nasi) (see Figs. 12-6 and 12-7) is a satellite of the lateral nasal artery. It is a tributary that enters the facial vein. The deep facial vein (v. faciei profunda) (Figs. 12-6 through 12-8) has no companion artery and is significant for its deep course and many anastomoses. A former name was vena reflexa (Preuss, 1954). It is 2 to 4 mm in diameter at its terminal end, which lies in the fascia cranial to the masseter muscle, approximately 1.5 cm ventral to the zygomatic arch. It arises in the ventral part of the orbit and the adjacent pterygopalatine fossa. The main portion of the vein arches dorsomedially and anastomoses with the ventral external ophthalmic vein on the floor of the orbit. An anastomosis with the superficial temporal vein frequently occurs as a small vein that obliquely crosses the lateral surface of the zygomatic arch. A small vein unites the deep facial with the maxillary vein by running across the lateral surfaces of the pterygoid muscles. Union of the sphenopalatine, infraorbital, and occasionally the major palatine veins may form a short venous trunk that enters the deep facial vein. The major palatine vein is small, if it is present at all. These veins are satellites of the comparable arteries. The main venous drainage of the hard palate is by a poorly formed venous plexus that is continuous with the much more salient venous plexus of the soft palate. Therefore the venous drainage of the hard and soft palates is not chiefly through satellites of the arteries supplying them, but by means of the veins of the palatine plexuses that drain into the right and left maxillary veins (Fig. 12-8). One or two veins consistently leave the ventral part of the ocular muscles to enter the deep facial vein. It also receives dental rami from superior cheek teeth and tributaries from the maxilla as it curves from the deep surface of the masseter muscle before entering the facial vein. The inferior labial vein (v. labialis inferior) (Fig. 12-6), a satellite of its artery, runs along the ventral border of attachment of the buccinator muscle. It receives an anastomosis from the submental vein and at its termination a vein that arises in the intermandibular space. This vessel runs along the margin of insertion of the digastric muscle, then over the lateral surface of the mandible. It may terminate in the facial vein. Throughout the course of the facial vein, small branches from the skin and fascia enter it. Ellenberger and Baum (1943) illustrate a small anastomotic vein located between the facial and the superficial temporal veins, as well as small branches coming from the mandibular lymph nodes. The submental vein (v. submentalis) (Figs. 12-5 and 12-6) receives tributaries from the mylohyoid and geniohyoid muscles as it courses caudally along the ventral portion of the body of the mandible. Its termination is variable as it may terminate in the facial vein, inferior labial vein or the hyoid venous arch. The lingual vein (v. lingualis) (Figs. 12-5, 12-6, and 12-8) is the ventral tributary that joins the facial vein to form the linguofacial vein. It begins in the apex of the tongue, and as it courses caudally it is augmented by numerous deep lingual tributaries from this organ. It lies in areolar tissue in association with the lingual artery and hypoglossal nerve, lateral to the genioglossal and medial to the hyoglossal muscles. Approximately 1 cm rostral to the body of the basihyoid bone it crosses the dorsal border of the hyoglossus muscle and comes to lie dorsal to the mylohyoid muscle. As it courses caudally from deep to the caudal border of the mylohyoid muscle it is joined by the sublingual vein (v. sublingualis). This vein begins in the rostral part of the lingual frenulum and runs caudally on the dorsal surface of the mylohyoid muscle. It lies directly deep to the thin mucosa between the lingual frenulum and the sublingual fold that lies lateral to the frenulum. It is occasionally used for venipuncture, but this is ill advised, as the exceedingly loose tissue that surrounds the vessel allows considerable hemorrhage to occur. Rostrally, this vein is accompanied by its satellite artery and the lingual branch of the mandibular nerve (V). It carries blood from the frenulum and the closely adjacent major sublingual and mandibular salivary ducts and the polystomatic part of the sublingual salivary gland. The hyoid venous arch (arcus hyoideus) (Figs. 12-5 and 12-6) is a constant, large, unpaired vein, approximately 3 mm in diameter and 3 to 4 cm long, which lies ventral to the basihyoid bone. It usually connects right and left lingual veins approximately 1 cm caudal to the termination of the sublingual veins. Petit (1929) illustrates this vessel as extending between the two sublingual veins. It may be double. It may receive the submental vein and on each side of the midline it receives the caudally running small submental branch (ramus submentalis), which usually begins as a single vessel in the midline between the fellow mylohyoid muscles. It receives delicate tributaries from both the mylohyoid and the geniohyoid muscles. Entering the caudal surface of the hyoid venous arch at the midline is the small unpaired laryngeal vein, v. laryngea impar. It anastomoses with the cranial laryngeal vein and usually with end tributaries of the thyroid veins. The cranial laryngeal vein (v. laryngea cranialis) (Figs. 12-5 and 12-6), a satellite of the like-named artery, leaves the larynx ventral to the cranial corner of the thyroid cartilage in company with the artery and cranial laryngeal nerve. It is usually a tributary of the ascending pharyngeal vein but may join the lingual vein approximately 1 cm from its termination. It may send a communicating branch to the internal jugular vein. The maxillary vein (v. maxillaris) (Figs. 12-5, 12-6, 12-8, and 12-22) begins ventral to the alar canal by a continuation and later a consolidation of the extension of the ophthalmic plexus. The formation and anatomy of the venation in this location are complicated and variable. Usually a small vein lies in the alar canal and receives an emissary vein of the round foramen (v. emissaria foraminis rotundi) from the cavernous sinus through the round foramen. Rostrally the vein in the alar canal joins the ophthalmic plexus, whereas caudally it joins the maxillary vein. Here also the maxillary vein receives an emissary vein from the oval foramen (v. emissaria foraminis ovalis) and the middle meningeal vein (v. meningea media) that is a satellite, usually double, of the corresponding artery. Approximately 5 mm caudal to the oval foramen, two more veins join the maxillary vein. One of these is small and comes from the pterygoid canal; the second is the larger emissary vein from the foramen lacerum (v. emissaria foraminis laceri) that passes through the foramen lacerum, and connects internally at the confluence of the ventral petrosal and cavernous sinuses. The maxillary vein winds laterally, caudal to the retroarticular process, and receives the vein of the palatine plexus. The venous palatine plexus (plexus venosus palatinus) (see Fig. 12-8) is a rather loose network of veins in the soft palate. The largest elements of this plexus are 0.5 mm in diameter. Rostrally the plexus anastomoses with the sphenopalatine and deep facial veins. The emissary vein of the retroarticular foramen (v. emissaria foraminis retroarticularis) (Figs. 12-6, 12-8, and 12-22) was formerly called the retroglenoid or retroarticular vein. It is a continuation of the temporal sinus that leaves the skull through the retroarticular foramen and more than doubles the size of the maxillary vein by joining it caudal to the temporomandibular joint. The intracranial formation of this vein is described with the veins of the central nervous system. The inferior alveolar vein (v. alveolaris inferior) (Fig. 12-6), formerly mandibular vein, is the satellite of the comparable artery. It leaves the mandibular foramen and at once receives a branch from the musculature medial to the mandible. Entering the maxillary vein approximately 5 mm caudal to the entry of the inferior alveolar vein is the masseteric vein (v. masseterica). This small tributary comes from the dorsal caudal border of the masseter muscle and curves medial to the caudal border of the mandible before it terminates. The superficial temporal vein (v. temporalis superficialis) (Fig. 12-6) is approximately 2.5 mm in diameter as it terminates in the dorsal surface of the maxillary vein. The vein crosses ventral to the base of the ear, deep to the parotid salivary gland. A dorsal tributary arises dorsomedial to the orbit by occasionally anastomosing with the small frontal vein, a tributary of the v. angularis oculi. A ventral tributary takes a dorsal course in the caudal part of the orbit. It runs deep to the deep temporal fascia, crosses medial to the orbital ligament, and continues medial to the zygomatic arch to anastomose with a branch of the deep facial vein. This anastomotic channel is more than 1 mm in diameter. A small, third anastomotic channel between the superficial temporal vein and the veins of the orbit is formed by a branch that runs through the rostral portion of the temporal muscle to enter the orbit and anastomoses with the ophthalmic plexus. The superficial temporal vein, after its formation by the three anastomotic branches, runs caudally deep to the temporal fascia. It receives numerous tributaries from the temporal muscle in its course toward the base of the ear. The rostral auricular vein (v. auricularis rostralis) is a small vein that begins in the interauricular musculature and skin and runs transversely, deep to the rostroauricular muscles, rostral to the base of the ear. It receives small branches from the skin and auricular muscles and the base of the pinna itself. The medial auricular vein (v. auricularis medialis) is a tributary to it. The rostral auricular vein terminates in the superficial temporal vein. The transverse facial vein (v. transversa faciei) is a small tributary that arises in the fascia ventral to the zygomatic arch. It empties into the superficial temporal vein approximately 1 cm ventral to the termination of the much larger rostral auricular vein. According to Ellenberger and Baum (1943), the rostral auricular vein terminates in the caudal auricular vein 50% of the time. As the superficial temporal vein grooves the rostral border of the parotid salivary gland, it receives one or more parotid branches from it. The caudal auricular vein (v. auricularis caudalis) (Figs.12-6 and 12-8) is formed by the lateral and intermediate auricular veins (vv. auricularis medialis et lateralis). The marginal medial and lateral auricular veins anastomose with each other near the apex of the pinna on the caudal, or convex, side. Unlike the caudal auricular artery, the caudal auricular vein anastomoses with the rostral auricular vein by means of a venous circle that lies on the cervicoauricular and interauricular muscles. This venous circle receives tributaries from the adjacent muscles. The caudal auricular vein receives the deep auricular vein (v. auricularis profunda) near the base of the ear and terminates in the maxillary vein caudal to the termination of the superficial temporal vein. A portion of the caudal auricular vein is bridged superficially by parotid salivary gland tissue and receives parotid branches (rami parotidei) from the gland. The deep auricular vein may enter the maxillary vein directly between the entry of the superficial temporal and caudal auricular veins. The right azygos vein (v. azygos dextra) (Figs. 12-1 and 12-9) develops in the dog. It is approximately 8 mm wide at its junction with the cranial vena cava where the latter terminates in the right atrium opposite the right third intercostal space. It begins on the median plane ventral to the body of the third lumbar vertebra by anastomosing with the single trunk formed by the merging of the right and left third lumbar intervertebral veins. Lying in the fat with the lumbar lymphatic trunk, it runs cranially through the aortic hiatus, flanked by the tendons of the crura of the diaphragm and the psoas major muscles. In the caudal third of the thorax it inclines slightly to the right, where it lies in the angle formed by the vertebral bodies and the aorta. Here, covered only by mediastinal pleura, it passes cranially to the base of the heart, hooks ventrally around the root of the right lung, and empties into the termination of the cranial vena cava at a right angle. It has the following tributaries: lumbar, dorsal costoabdominal, dorsal intercostal, and bronchoesophageal veins. The first two lumbar veins are smaller than the others. They are received by the initial part of the azygos vein as it extends cranially from an anastomosis with the stem, which receives the right and left third lumbar intervertebral veins. The initial part of the azygos vein may be double as it forms this union. The azygos vein carries most of the blood from the vertebral venous plexus via the dorsal intercostal and lumbar veins to the cranial vena cava (Bowsher, 1954). The intervertebral veins of the thorax are single vessels that join the dorsal intercostal veins at the highest points of the several intercostal spaces. The lumbar intervertebral veins are double as they traverse the intervertebral foramina. They then quickly unite to form the several lumbar veins (Worthman, 1956). The veins of the thoracic limb may be divided into superficial and deep sets. The cephalic vein (v. cephalica) (Figs. 12-1, 12-4, 12-11 and 12-12) is a tributary of the external jugular vein. It is the only large superficial vein of the thoracic limb. It begins on the mediopalmar surface of the carpus where it is a continuation of the radial vein. Distal to this the radial vein arises from the superficial palmar arch (arcus palmaris superficialis) that crosses the palmar side of the distal third of the second to fifth metacarpal bones and drains the palmar common digital veins (vv. digitales palmares communes). Here this arch is well protected by the heavy metacarpal pad. The radial vein (v. radialis) (Fig. 12-12) leaves the superficial arch and runs proximally on the palmar side of the interosseous muscles directly caudal to the interosseous space between the second and third metacarpal bones. It passes superficial to the flexor retinaculum, formerly called the palmar carpal transverse ligament, parallel to the carpal canal. The cephalic vein arises here from the radial vein as the main conduit of venous blood from the palmar surface of the paw. The smaller radial vein continues proximally in the antebrachial muscles. The cephalic vein usually receives three tributaries in the antebrachium. On gaining the cranial surface of the antebrachium, it is known as the antebrachial part of the cephalic vein. From the carpus it runs proximally until it reaches the cranial surface of the m. extensor carpi radialis, and then it follows this muscle to the flexor angle of the elbow joint. One of these tributaries comes from a band of skin extending to the elbow, whereas the other two are tributaries from the flexor muscles of the antebrachium. It is flanked on its medial and lateral sides by the medial and lateral branches of the superficial antebrachial artery as well as by the medial and lateral branches of the superficial radial nerve. It is 3 to 5 mm in diameter and lies directly deep to the skin, loosely surrounded by the superficial fascia. Because of its size, location, and ease of compressibility, it is the favored site for venipuncture in the dog. The antebrachial part of the cephalic vein is augmented by receiving the accessory cephalic vein (v. cephalica accessoria) at the beginning of the distal fourth of the antebrachium. This vein, approximately 2 mm in diameter at its termination, begins on the dorsum of the metacarpus where it receives dorsal common digital veins II, III, and IV (vv. digitales dorsales communes II-IV) and passes proximally over the carpus and the cranial aspect of the distal portion of the antebrachium before joining the cephalic vein. It is joined by dorsal common digital vein I (v. digitalis dorsalis communis I) from the first digit and skin of the second metacarpal bone at the distal end of the antebrachium. The median cubital vein (v. mediana cubiti) (Figs. 12-4, 12-10, and 12-11) extends between the brachial or superficial brachial vein at the flexor angle of the elbow joint and the cephalic vein of the arm. It is approximately 2 mm in diameter and 2 cm long. It crosses the distal end of the m. biceps brachii obliquely as it runs proximolaterally to anastomose with the cephalic vein near the lateral border of the biceps muscle. The brachial part of the cephalic vein continues the antebrachial part from the flexor angle of the elbow joint. It runs proximally, crosses the cleidobrachialis muscle, and joins the axillobrachial vein on the lateral surface of the triceps muscle. The cephalic vein runs proximomedially deep to the cleidobrachialis muscle at the junction of the middle and distal thirds of the brachium. It enters the external jugular vein between the omobrachial and the axillary veins and receives a tributary from the major tubercle of the humerus and two or three more from the brachiocephalicus and pectoral musculature. This connection of the cephalic vein to the external jugular vein was formerly known as the distal communicating branch. Gómez et al. (2007) describe the bilateral absence of the brachial part of the cephalic vein in one dog, and the bilateral absence of the omobrachial vein in two dogs. The axillobrachial vein (v. axillobrachalis) (Figs. 12-1, 12-4, and 12-10), formerly considered a continuation of the cephalic vein, courses over the lateral head of the triceps muscle and at the distal border of the m. deltoideus passes caudal to the humerus. Caudal to the shoulder joint, the axillobrachial vein anastomoses with both the axillary and the subscapular veins. It receives large tributaries from the triceps muscle in its course through it and terminates in the axillary vein. The radial vein (v. radialis) (Fig. 12-12) arises from the superficial and deep palmar venous arches (arcus palmaris superficialis and arcus palmaris profundus). The majority of the venous blood from the superficial arch flows through the anastomosis of the radial vein with the cephalic vein. The small radial vein follows the mediocaudal border of the radius covered by antebrachial fascia. It joins the median vein distal to the deep antebrachial vein. The ulnar vein (v. ulnaris) (Figs. 12-1 and 12-12) accompanies its corresponding artery and arises from its union with the palmar branch of the caudal interosseous vein in the carpal canal. It passes proximally in the deep digital flexor muscle, receiving tributaries from most of the caudal antebrachial muscles. It joins the brachial or common interosseous vein in the proximal antebrachium. The small median vein (v. mediana) (Figs. 12-1 and 12-4) accompanies the corresponding artery. It arises from the superficial palmar venous arch, passes proximally through the carpal canal and in the middle to proximal antebrachium is joined by the radial vein and deep antebrachial vein (v. profunda antebrachii). Proximal to this, it is continued by the brachial vein. The brachial vein (v. brachilis) (Figs. 12-1 and 12-4) receives the relatively large common interosseous vein (v. interossea communis) with its ulnar and cranial and caudal interosseous branches. At the elbow the large median cubital vein connects the brachial vein or superficial brachial vein with the cephalic vein. In the brachium, the brachial vein receives the transverse cubital (v. transversa cubiti), superficial brachial (v. brachialis superficialis), collateral ulnar (v. collateralis ulnaris), bicipital (v. bicipitalis) and deep brachial (v. profunda brachii) veins. Proximal to this the brachial vein is continued by the axillary vein. The axillary vein (v. axillaries) (Figs. 12-1, 12-2, 12-4, 12-13) receives the small cranial circumflex humeral vein (v. circumflexa humeri cranialis) cranially and the thoracodorsal vein (v. thoracodorsalis) caudally. A large subscapular vein (v. subscapularis) with its caudal circumflex humeral vein (v. circumflexa humeri caudalis) joins the axillary vein caudal to the shoulder. Proximal to this, a small lateral thoracic vein (v. thoracica lateralis) enters caudally and an external thoracic vein (v. thoracica externa) enters cranially. The axillobrachial vein connects the cephalic vein superficially with the axillary or caudal circumflex humeral vein caudal to the shoulder joint. At the first rib the axillary vein becomes the subclavian vein and joins the external jugular vein to form the brachiocephalic vein.
Veins
General Considerations
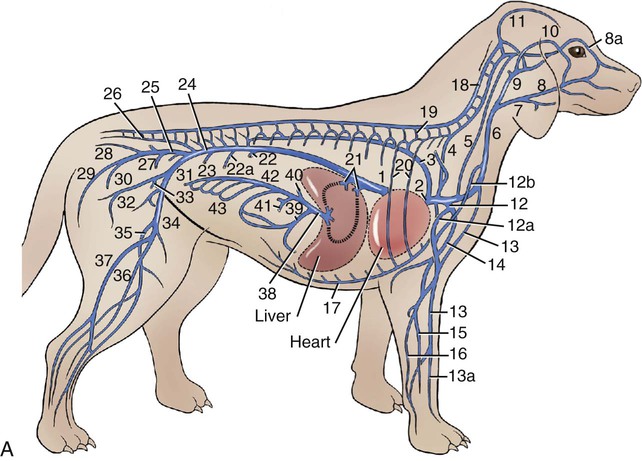
(From Evans HE, de Lahunta A: Miller’s guide to the dissection of the dog, ed 7, Philadelphia, 2010 Saunders.)
Cranial Vena Cava
Azygos System of Veins
Veins of the Thoracic Limb
Superficial Veins of the Thoracic Limb
Deep Veins of the Thoracic Limb
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Veins
Only gold members can continue reading. Log In or Register to continue
