Palle Brink, John Schumacher
Uteropexy in Older Mares
Normally, mares are resistant to uterine infection after breeding, even though the endometrium is subjected to the inflammatory effects of debris and bacteria deposited in the uterus during copulation. Mares unable to clear the deposited debris and bacteria from the uterus are susceptible to uterine infection. In susceptible mares, the uterus is oriented more vertically within the abdominal cavity than its normal horizontal position. This detrimental change in uterine position results from stretching of the mesometrium from the weight of foals during numerous pregnancies. Contractions of a horizontally oriented uterus successfully push the contaminated uterine fluid and debris dorsally and caudally, causing it to exit the uterus, but the strength of contractions of a ventrally oriented uterus may be inadequate to clear the uterus of debris and bacteria that incite inflammation. A ventrally oriented uterus can be returned to a normal, horizontal orientation by imbricating the two mesometria that suspend the uterine body and each horn. By returning the uterus to its normal horizontal position, uterine clearance may improve, which may improve fertility.
The surgery to resuspend the uterus in a horizontal orientation (i.e., uteropexy) has been described in detail elsewhere (Brink et al, 2012), but a brief description of the laparoscopic surgery follows. Uteropexy can usually be performed without insufflating the abdomen if the mare is held off feed for at least 36 hours. Presurgical treatment with an analgesic agent such as flunixin meglumine may prevent postoperative abdominal discomfort. The mare is sedated with detomidine hydrochloride (0.005 to 0.01 mg/kg, IV) and butorphanol tartrate (0.01 to 0.02 mg/kg, IV) administered as a bolus. Administration of these drugs can be repeated if necessary, or sedation can be maintained at a more constant level by using continuous rate infusion after administering a loading bolus of the sedative detomidine (0.02 mg/kg/hour) and butorphanol (0.012 mg/kg/hour).
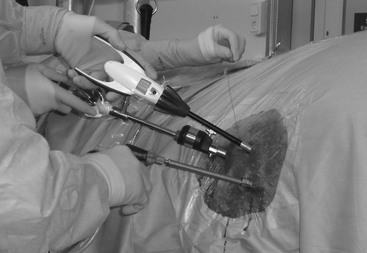
Three trocar-and-cannula assemblies are inserted in the flank to use as portals to insert the laparoscope and instruments for visualizing and accessing the mesometrium. An injection cannula is used to administer local anesthetic solution into the mesometrium to minimize painful reactions in response to manipulation of the mesometrium and uterus. The left mesometrium is imbricated first, to allow the cecum to fall from the right paralumbar fossa as negative pressure within the abdominal cavity is relieved when the portals are placed through the left flank. This makes inadvertent puncture of the cecum less likely when portals are introduced through the right flank. Portal sites for mesometrial imbrication are the 17th intercostal space, slightly below an imaginary line drawn horizontally through the ventral border of the tuber coxae (i.e., the cranial portal), a site midway between the ventral aspect of the tuber coxae and the last rib at the dorsal level of the crus of the internal abdominal oblique muscle (i.e., the middle portal), and a site 6 cm ventral and 2 cm caudal to the central portal (i.e., the caudal portal) (Figure 166-1). The mesometrium is imbricated with a laparoscopic needle holder or an endoscopic automated suturing device1 (Figure 166-2). To imbricate the mesometrium, the body of the uterus is sutured to the dorsal aspect of the mesometrium with a simple-continuous suture pattern by passing the needle through the seromuscular layers of the body of the uterus near the juncture of the uterus with the mesometrium and then through the dorsal aspect of the mesometrium. Suturing begins close to the cervix and extends caudally to end near the tip of the uterine horn. Tissue drag created by absorbable or nonabsorbable multifilament suture material tends to hold the imbricated tissues in apposition while subsequent suture bites are inserted (Figure 166-3). Sutures are placed approximately 1.5 cm apart, and about 10 to 14 suture bites through the seromuscular portion of the uterus and the mesometrium are needed to elevate one side of the uterus. Silk may be preferred to absorbable suture by some surgeons because it is more likely to create adhesions (Figure 166-4), which add strength to the line of apposed tissue and is less expensive than absorbable suture used with the Endo Stitch1 device. The region of the mesometrium through which the needle is passed should be sufficiently dorsal to the uterus to elevate the uterus to a horizontal position when the suture is tightened.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


