CHAPTER 52 Urological Interventional Techniques in the Feline Patient
BACKGROUND—INTERVENTIONS IN HUMAN UROLOGY
In human urology the development and improvements in ureteroscopy, ureteral stenting, extracorporeal shockwave lithotripsy (ESWL), laser lithotripsy, laparoscopy, and percutaneous nephroureterolithotomy (PCNUL) have almost eradicated the need for open urinary surgery for stone disease, strictures, trauma, or neoplasia. Currently, ureteroscopy is the first-line evaluation of ureteral neoplasia, upper tract essential hematuria, ureteral calculi larger than 5 mm, and evaluation for ureteral obstructions. Cystoscopy is the standard diagnostic tool for human patients with dysuria because it can provide both diagnostic and treatment options. Ureteroliths smaller than 5 mm have a 98 per cent chance of spontaneous passage with medical management alone.1,2 For larger stones, or those that do not pass spontaneously, ESWL is effective in 50 to 81 per cent of cases, although most of the literature suggests that this number is closer to 50 to 67 per cent.1,2 Ureteroscopy has a near 100 per cent success rate when Holmium:YAG laser lithotripsy is used.3–7 PCNUL has been successful for large proximal impacted ureteral stones.8 Ureteral stenting was first introduced in 1967 for evaluation of human patients with malignant ureteral obstructions.9 Stents still are widely used to treat both benign and malignant obstructive disease and this is considered standard-of-care.9–15 Ureteral stenting for stone disease typically is done after ureteroscopy for postscoping spasm and edema, and in children, it has been performed routinely prior to ureteroscopy to allow for passive ureteral dilation in anticipation of immediate ureteral bypass, spontaneous stone passage, and the ease of extracorporeal shockwave lithotripsy.9–15 Ureteral stenting also has been shown to ease a future ureteroscopy dramatically in a small pediatric ureter.15 Percutaneous cystolithotomy (PCCL) often is the treatment of choice for large cystic stone burdens, in which repetitive urethral trauma is a concern for transurethral lithotripsy.16
EQUIPMENT
LITHOTRIPSY
Multiple types of intracorporeal lithotrites and lasers are available including ultrasonic, pneumatic, electrohydraulic, and holmium:YAG lasers, which can be used for stone fragmentation, and a diode laser that is used most often for tissue coagulation or resection (i.e., lasering intramural ureteral ectopia). Extracorporeal shock wave lithotripsy (ESWL) also has application for small to moderate size ureteral calculi in cats, but success has been variable with stone passage in feline patients, when compared with dogs.17–19
URINARY ACCESS (GUIDEWIRES, CATHETERS, AND STENTS)
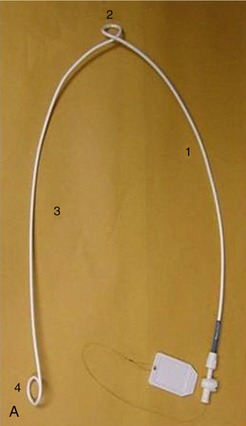
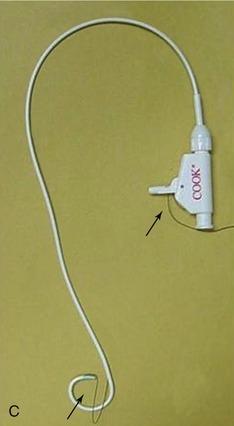
Guidewires of various sizes, shapes, and stiffness are needed for each procedure. Urinary catheters and stents can be used for various purposes to divert urine throughout the entire urinary collection system. Catheters are defined as flexible or rigid hollow tubes employed to drain fluids from body cavities. Most catheters in the urinary system are used for temporary drainage of the renal pelvis (nephrostomy tubes), ureter, or urinary bladder (cystostomy tubes). Urinary catheters are classically soft, comfortable, polyurethane type tubes with an open lumen, permitting temporary drainage. Stents are defined as small tubes, often expandable, inserted across a blocked lumen to restore patency. Urinary stents typically are used for permanent or long-term diversion in the kidney, ureter, bladder, or urethra. Stents most often are completely indwelling tubes that can be placed for various purposes, most commonly to bypass a malignant obstruction, stricture, or embedded stone (i.e., ureterolithiasis). Stents come in different materials (e.g., metal, polyurethane, plastic, rubber), shapes, and sizes (Figure 52-1).

DISEASES OF THE UPPER URINARY COLLECTION SYSTEM: RENAL PELVIS AND URETER
Feline ureterolithiasis is the most common upper urinary tract frustration that requires immediate intervention. Other causes for ureteral obstruction include ureteral strictures/stenosis and ureteral neoplasia. Greater than 98 per cent of feline ureteroliths were recently documented to be composed of calcium oxalate, which is a trend from earlier decades. This means that these stones will not dissolve medically, and either need to pass spontaneously, remain in place, or be removed. Once medical management fails (traditionally: intravenous fluid therapy, mannitol CRI [constant rate infusion], and alpha-adrenergic blockade ± amitriptyline), partial obstructions often are monitored and left in the ureter, considering the risk-benefit ratio of attempted surgical removal. If there is a complete ureteral obstruction, decompression of the renal pelvis becomes imperative in order to preserve renal function to the ipsilateral kidney. After a ureteral obstruction, studies in dogs have shown the ureteral pressures increase immediately and can take over 24 hours after obstruction relief for the pressure to decline.20 After a transient increase in pressure the renal blood flow diminishes to 40 per cent of normal over the first 24 hours, but drops to 20 per cent of normal by 2 weeks.21,22 This increase in pressure generated by the ureteral obstruction is transmitted to the entire nephron and a decrease in glomerular filtration rate (GFR) occurs via concurrent vasoactive mediator release, leukocyte influx, and subsequent fibrosis.21 The longer the ureter remains obstructed, the more damage occurs, which is irreversible. In a study of normal dogs it was found that after 7 days of obstruction, the GFR was permanently diminished by 35 per cent, and when the obstruction lasted for 14 days, the GFR was diminished by 54 per cent.21,23–25 These numbers were in a dog model without preexisting azotemia, chronic interstitial nephritis, or chronic obstructions, so extrapolation of a worse outcome might be expected in our feline patients, making aggressive and timely intervention worth considering.
Traditional intervention has been accomplished surgically via ureterotomy, neoureterocystostomy, ureteronephrectomy, and renal transplantation. Kyles et al recently reported two retrospective studies in a large number of cats.26,27 There were high procedure-associated complications (over 30 per cent) and mortality (18 to 39 per cent depending on the type of management) documented. This study was from two universities with extensive experience with ureteral surgery. The morbidity and mortality may be even higher in environments in which operating microscopes and microsurgical experience are not as available. Many of the associated complications with surgery are caused by site edema, recurrence of stones that pass from the renal pelvis to the surgery site, stricture formation, and ureterotomy-associated or nephrostomy tube–associated urine leakage.26,27 Over 10 per cent of cats who survived their complications required a second surgical procedure during the same visit, and 30 per cent of those cats subsequently were euthanized or died for serial complications associated with their ureteral stones/surgeries.26 Of the large number of cats in that study, a relatively small number had long-term imaging follow-up, and 40 per cent of those who underwent subsequent imaging had evidence of ureteral stone recurrence, of whom 85 per cent had evidence of nephrolithiasis at the time of the first ureteral surgery.26 The number of cats who did not have stone recurrence with prior nephrolithiasis was not evident in that study. Chronic renal failure is common at the time of diagnosis (>75 per cent were azotemic with a unilateral obstruction), and persistent azotemia is a widespread problem after a successful intervention (over 50 per cent of cats).26,27 However, in spite of all of the surgical concerns, the survival rates were dramatically higher for cats who had intervention performed, when compared with those patients treated with medical management alone. Medical management has been shown to be effective in a minority of cases,26 but should be considered prior to any intervention, particularly for stones in the distal one-third of the ureter, and for stones smaller than 2 to 3 mm. Finding a less invasive alternative that results in immediate decompression and stabilization of associated azotemia, and allows patency to be established concurrently would be ideal, and in human beings minimally invasive treatments have replaced open surgery.1–15 The placement of a double pigtail ureteral stent, either minimally invasively (IR technique) or surgically, could potentially circumvent the complications of surgery alone (e.g., leakage, stricture, re-obstruction), and quickly and efficiently stabilize the patient while decreasing renal pelvic pressure and stopping the cycle of pressure-induced nephron death and renal fibrosis.
URETERAL STENTING
Ureteral stenting has been performed for a variety of disorders in dogs and cats.28,29 The goals of ureteral stenting include (1) to divert urine from the renal pelvis into the urinary bladder to bypass a ureteral obstruction (e.g., ureterolithiasis, obstructive neoplasia, ureteral stricture/stenosis), (2) to encourage passive ureteral dilation (for ureteral stenosis/strictures or future stone passage), (3) to decrease surgical tension on the ureter after/during surgery (i.e., resection and anastomosis or proximal ureteral re-implantation) and prevent postoperative leakage or edema, and (4) to aid in extracorporeal shockwave lithotripsy for large obstructive ureteroliths or nephroliths that could result in serial ureteral obstructions if the stones do not pass completely down the ureter (steinstrasse).1
The first report of ureteral stent placement was in 1967 in a human patient for malignant obstruction.9 Since that time nonresectable trigonal or ureteral tumors are treated similarly, with an indwelling double pigtail ureteral stent used to bypass the obstruction. These tumors are accessed more easily through an antegrade percutaneous approach, in order to gain access down the ureter, an observation we have appreciated in veterinary patients as well. In human beings there is a 96 to 98 per cent success rate in stent placement with this antegrade approach.9–12 It was not until 1977 that a report of ureteral stenting for benign disease was published, for a ureteral stricture.12 Then, in 2005 ureteral stenting was described in pediatric urology as a means to facilitate ureteroscopic procedures.15 Stents encouraged passive dilation of the ureter, a finding that has been reproduced in dogs.13 The stent is left in place for several weeks, enabling spontaneous voiding of ureteroliths or the subsequent passage of a ureteroscope in such small patients.13,15 However, few reports of clinical investigation or application of ureteral stents in dogs or cats have been published.27,28 At the author’s institution, over 90 dog or cat ureters have been stented for various clinical purposes.
Ureteral stents are used classically to bypass obstructions from ureterolithiasis, malignant obstructive neoplasia, trauma, and ureteral stenosis or stricture. A ureteral stent can be placed after interventional procedures (such as ureteroscopy, ureteral balloon dilation, or lithotripsy) in order to prevent temporary obstruction from ureteral edema or spasm; following surgical ureterotomy, ureteral resection, and anastomosis; when there is a ureteral tear; to provide tension relief and healing; to prevent postoperative ureteral leaking; and to prevent ureteral stricture formation while the surgical site heals. Some people believe ureteral stents also are ideal in patients with large nephroliths (>10 to 15 mm) or ureteroliths (>4 to 5 mm) who are undergoing ESWL to aid in ureteral stone localization and stone fragment passage after the ESWL treatment.13,14,17,18 Ureteral stenting has been performed in cats with large numbers of obstructive nephroliths, in order to maintain urine flow and to prevent entry of nephroliths into the proximal ureter.
Ureteral Stents
There are three main types of ureteral stents/catheters: (1) an indwelling double pigtail ureteral stent (vet stent, double pigtail ureteral stent, Infiniti Medical LLC, Malibu, CA), which is the most common type used in veterinary and human medicine, (2) a nephroureteral stent (nephroureteral catheter, Cook Medical, Bloomington, IN), and (3) locking loop pigtail catheter (Dawson-Meuller drainage catheter, 5 Fr, Cook Medical, Bloomington, IN; Infiniti 6 Fr locking loop drainage catheter, Infiniti Medical LLC, Malibu, CA) (see Figure 52-1). The double pigtail stent, which is the stent of choice in cats, is completely intracorporeal and can remain in place for months or years if necessary (recommended for <6 months, but the author has experience with >2 years of stent patency in cats and dogs). Each loop of the pigtail is curled (one in the bladder and one in the renal pelvis), allowing for direct urinary diversion from the kidney to the urinary bladder, around the stones, or through the stricture (Figure 52-2).


In female cats ureteral stents most often are placed either cystoscopically or via a cystotomy; in retrograde manner, the stent can be advanced through the ureteral orifice at the ureterovesicular junction. Retrograde placement also can be accomplished during surgical cystotomy. Ureteral stents also can be placed antegrade through the renal pelvis (percutaneously or surgically), or surgically during ureterotomy. Under general anesthesia the retrograde technique uses cystoscopy and concurrent fluoroscopy. An angle-tipped hydrophilic guidewire (0.018″ Weasel wire) (Weasel Wire [0.035″, 0.025″, 0.018″] hydrophilic angle-tipped guidewire, Infiniti Medical LLC, Malibu, CA) is advanced into the distal ureter from the ureterovesicular junction. The wire is advanced up the length of the ureter and curled into the renal pelvis. Care is taken to bypass the obstruction carefully without perforating the ureter (see Figure 52-2). An open-ended ureteral catheter (open-ended ureteral catheter, 3 French, Cook Medical, Bloomington, IN) then is advanced over the wire under fluoroscopic guidance, and the guidewire is removed. A retrograde contrast ureteropyelogram is performed to help identify any lesions, stones, or filling defects in the ureter or renal pelvis. The wire is re-advanced through the catheter into the renal pelvis and the catheter is withdrawn. An indwelling double pigtail ureteral stent (vet stent, double pigtail ureteral stent, Infiniti Medical LLC, Malibu, CA) is placed over the guidewire under fluoroscopic guidance, with one curl remaining in the renal pelvis in front of the obstruction and the other in the urinary bladder. In cats this typically is a 12 cm, 3-Fr double pigtail multifenestrated stent (vet stent, double pigtail ureteral stent, Infiniti Medical LLC, Malibu, CA).
As described for retrograde placement of a ureteral stent, a guidewire is advanced up the ureteral orifice using cystoscopic and fluoroscopic guidance. An open-ended ureteral catheter is advanced over the wire and the wire subsequently is removed. Contrast media then is injected through the catheter to create mild ureteral distension and adequate visualization. Injections of contrast media can be repeated safely to confirm subtle lesions (see Figure 52-2).
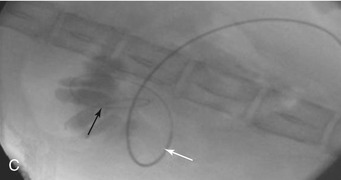
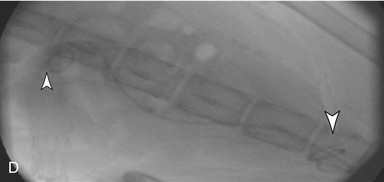
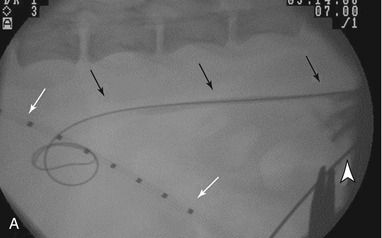
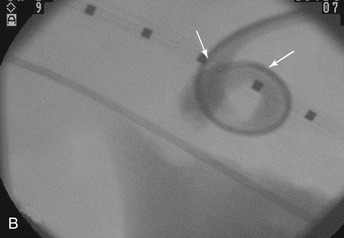
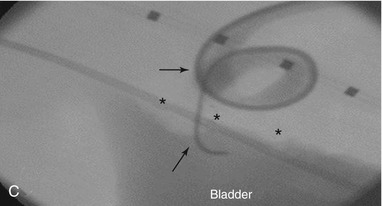
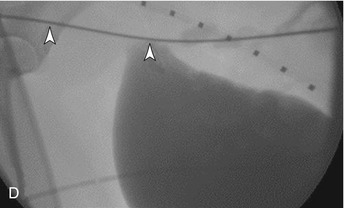
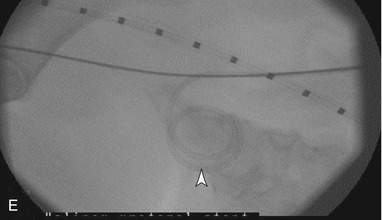
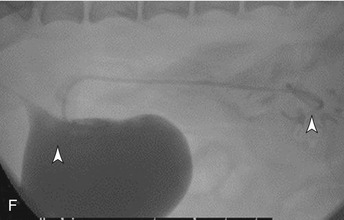
The antegrade technique, the preferred technique for male cats, requires percutaneous renal access with a renal access needle (21-gauge) (disposable trocar needle, 21 g × 7 cm, Cook Medical, Bloomington, IN) or over-the needle catheter (22-gauge). This can be done with either ultrasound or fluoroscopy. The guidewire is passed down the ureter, into the urinary bladder and out the urethra to have through-and-through access (“flossed”). This approach also is employed for ureteral obstruction by a bladder mass, when the ureteral orifice can not be identified cystoscopically (Figure 52-3). The stent then is placed in a retrograde fashion over the wire, as described above, to keep the hole in the kidney as small as possible (Figure 52-4).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


