Chapter 9 Urolithiasis
Introduction, Terminology, and General Pathophysiology
Urine Is a Complex Solution Containing Many Organic and Inorganic Solutes
1. More of a given solute can remain in solution in urine than in water because of the complex interactions that occur among the various organic and inorganic constituents in urine.
2. For several possible reasons (e.g., diet, decreased water intake, altered urine pH, relative lack of inhibitors, or presence of promoters of crystallization), the solubility product of a particular solute may be exceeded, crystals may form, and these crystals may aggregate and grow. (Figure 9-1.)
a. If the crystals precipitate spontaneously, the process is called homogenous nucleation. Homogenous nucleation probably does not occur in urine.
b If another substance (e.g., desquamated epithelial cells, inflammatory cells and debris, bacteria, foreign body) acts as a nidus for crystal precipitation, the process is called heterogenous nucleation.

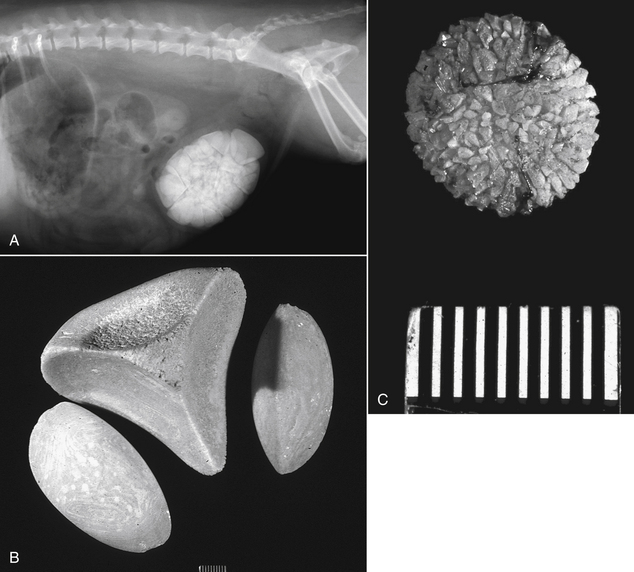
FIGURE 9-1 Note lamellar pattern of large urolith shown on radiograph after stone had been removed surgically.
 Most uroliths are identified in the lower urinary tract.
Most uroliths are identified in the lower urinary tract.a. When 70% or more of the urolith is composed of one type of crystalloid it is named for that crystal. Secondary crystalloids can comprise up to 30% of the total weight. Most stones in dogs and cats have one major crystal component (Figures 9-2 and 9-3). More than 90% of stones submitted for quantitative analysis are collected from the lower urinary tract.
b. When less than 70% of the urolith is composed of one mineral but without identifiable nidus, shell, or surface crystals, it is called a mixed urolith.
Urine Is Commonly Supersaturated With Crystalloids
1. Urine is commonly supersaturated with crystalloids, and observation of individual crystals does not necessarily mean the patient is at risk for urolithiasis. Cooling of the urine specimen during storage promotes in vitro crystal precipitation, and observed crystals may not have been present at the time the sample was collected. Supersaturation of urine with crystalloids depends on:
Amount of solute ingested and excreted
Promoters of Urolithiasis
Inhibitors of Urolithiasis
b. Inhibitors of aggregation include pyrophosphate, citrate, diphosphonates, and glycosaminoglycans (GAGs).
c. A urinary inhibitor of crystal growth called nephrocalcin is biochemically altered in some humans who develop calcium oxalate stones, and a similar change may occur in some affected dogs. Tamm-Horsfall mucoprotein normally protects against crystal aggregation in urine, but in some human patients it may self-aggregate and fail to protect against crystal aggregation.
Three General Theories of Urolithiasis
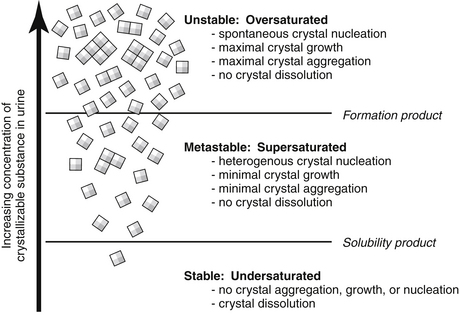
FIGURE 9-4 Crystal dissolution, formation, and growth as a function of the concentration of crystalloids.
 Calculi collected from the lower urinary tract are assumed to have formed there.
Calculi collected from the lower urinary tract are assumed to have formed there.2. The matrix-nucleation theory implies that some abnormal substance in the urine is responsible for the initial development of calculi.
3. The crystallization-inhibition theory suggests that the absence of some critical inhibitor (or presence of a promoter) of crystal formation is the primary factor in the development of calculi.
5. It has been assumed that calculi initially identified in the lower urinary tract actually formed in that location, but this has not been proven. Based on recent data about urolith formation in human patients, it is thought that uroliths may originate from abnormal processes in the kidneys themselves.
Pathophysiology of Individual Stone Types
Struvite Urolithiasis
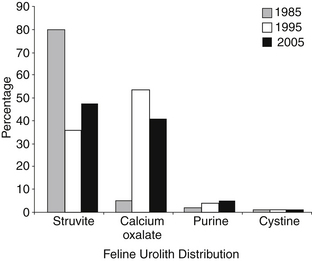
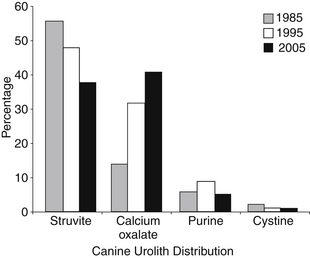
1. For many years, struvite was the most common type of urolith found in dogs and cats comprising 60% to 70% of uroliths in dogs and up to 95% of uroliths found in cats. Between 1981 and 2001, the frequency of calcium oxalate urolithiasis increased and that of struvite decreased. Today, struvite comprises 40% to 50% of uroliths in dogs and cats. The increase in calcium oxalate urolithiasis began to level off between 1998 and 2001. (see Figures 9-2 and 9-3.)
2. The major crystalloid in these uroliths is MgNH4PO4∙6H2O (struvite). Calcium phosphate as carbonate apatite often is present in small amounts (2%-10%). The presence of three cations (i.e., Ca+2, Mg+2, and NH4+) detected by early qualitative analytical methods was responsible for the name “triple phosphate” previously used for these stones. They also have been called magnesium ammonium phosphate stones.
3. Struvite uroliths are spherical, ellipsoidal, or tetrahedral in shape and may be present singly or in large numbers of varying sizes. (see Figure 9-5.)
4. In dogs and cats, the bladder is the most common site of struvite uroliths, although they may occur at any site in the urinary tract.
 Most dogs with struvite urolithiasis have underlying UTI that promotes urolith growth. Most cats with struvite urolithiasis have sterile urine when their calculi are first recognized.
Most dogs with struvite urolithiasis have underlying UTI that promotes urolith growth. Most cats with struvite urolithiasis have sterile urine when their calculi are first recognized.6. Infection of the urinary tract by urease-positive bacteria (especially staphylococci and Proteus sp) plays the most important role in the pathogenesis of struvite urolithiasis in dogs. More than 95% of dogs with struvite urolithiasis have infection as an underlying cause for the urolith growth. In almost all cats with struvite urolithiasis, infection is not present and the calculi are thought to be metabolic in origin. However, a family of Cocker spaniels with recurrent sterile struvite urolithiasis has been reported.
a. The solubility of struvite is markedly reduced in alkaline urine. Struvite becomes progressively less soluble as the pH increases above 6.7.
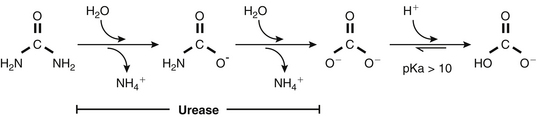
b. Hydrolysis of urea by urease-positive bacteria liberates ammonia and carbon dioxide, which alkalinizes the urine and increases availability of ammonium and phosphate ions for struvite crystal formation (Figure 9-6).
7. Struvite solubility is decreased in animals with persistently alkaline urine even in the absence of UTI. In dogs that form struvite stones in the absence of UTI, predisposing factors that may be associated with alkaline urine (e.g., family history of struvite stones, diet based on vegetable proteins, distal renal tubular acidosis) should be considered.
8. UTI usually is not present in cats with struvite stones. More than 95% of cats with struvite urolithiasis have sterile urine.
9. Diets formulated with high magnesium, phosphorus, calcium, chloride, or fiber, and moderate protein content are associated with increased risk of struvite urolithiasis in cats. Diets with high fat content, low in sodium or potassium, and those formulated to maximize urine acidity are associated with decreased risk of struvite urolithiasis in cats.
Oxalate Urolithiasis
1. Calcium oxalate stones are the most common type of urolith in humans, and their frequency has increased in dogs and cats and during the past 25 years.
2. Risk factors for development of oxalate urolithiasis in dogs.
a. Age older than 4 years. Affected dogs are older than 1 year of age and the highest risk occurs between 8 and 12 years of age. The average age of occurrence is between 8 and 9 years.
c. Breeds at highest risk are miniature and standard Schnauzer, Lhasa apso, Yorkshire terrier, Bichon frise, Shih tzu, miniature and toy poodle. Golden retriever, German shepherd, and Cocker spaniel are at lowest risk for oxalate urolithiasis.
3. Risk factors for development of oxalate urolithiasis in cats.
a. The increase in frequency of oxalate urolithiasis in cats over the past 25 years does not seem to be related to changes in the age, breed, sex, or reproductive status of the cat population during this time.
b. Exclusive feeding of an acidifying diet without provision of different brands of food or table scraps is a strong risk factor for development of calcium oxalate urolithiasis in cats.
e. Persian, Himalayan, Ragdoll, Havana Brown, and Scottish Fold breeds are at increased risk for development of oxalate urolithiasis whereas Siamese and Abyssinian cats are at decreased risk.
4. Calcium oxalate stones are composed of calcium oxalate monohydrate (whewellite) or calcium oxalate dihydrate (weddellite). Oxalate often is not detected by qualitative analysis, and quantitative analysis of stones is necessary for reliable identification.
5. Calcium oxalate calculi usually are white in color and very hard. They often have sharp, jagged edges and may be single or multiple in number. (see Figure 9-7.)
6. Oxalate stones often are found in the bladder and urethra, but they also are the most common type of urolith found in the kidney and ureter of both dogs and cats. A 10-fold increase in urolithiasis in the upper urinary tract of cats has been reported over the past 25 years.
8. Oxalate is derived both from the diet and endogenously from the metabolism of ascorbic acid (vitamin C) and the amino acid glycine. In human beings, increased dietary oxalate, increased gastrointestinal absorption of oxalate, vitamin B6 deficiency, and inherited defects of oxalate metabolism can predispose to development of calcium oxalate stones. The role of such factors in development of calcium oxalate stones in animals is not known.
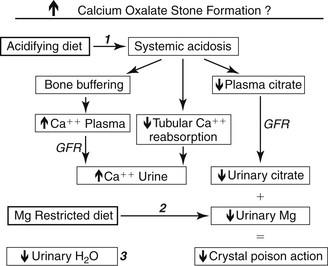
9. Altered calcium metabolism may play a role in development of oxalate urolithiasis (Figure 9-8).
a. Increased urinary excretion of calcium (hypercalciuria) can result from increased absorption of calcium from the intestinal tract (absorptive hypercalciuria), from increased urinary loss of calcium (renal leak hypercalciuria), or from increased release of calcium from bone (resorptive hypercalciuria). In absorptive as compared to renal leak hypercalciuria, urinary calcium excretion is higher after feeding than during fasting.
b. In one study, miniature Schnauzers had higher urinary calcium excretion during fasting than did beagles and urinary calcium excretion increased 3-fold after feeding (i.e., hypercalciuria seemed to be absorptive).
c. Dogs or cats with hypercalcemia due to primary hyperparathyroidism may develop calcium oxalate or calcium phosphate uroliths due to parathyroid hormone-mediated mobilization of calcium from bone (resorptive hypercalciuria).
d. Chronic acidosis may be associated with increased urinary excretion of calcium due to increased calcium release from bone as a buffering mechanism. Long-term feeding of an acidifying diet may contribute to this resorptive hypercalciuria and may partially explain the increase in calcium oxalate urolithiasis in cats during the past 25 years (i.e., increased feeding of acidifying diets to prevent struvite urolithiasis). Decreased magnesium concentration in the urine also may contribute, because magnesium is a crystal inhibitor for calcium oxalate.
e. Dogs with hyperadrenocorticism are predisposed to development of calcium oxalate and calcium phosphate uroliths possibly as a result of decreased renal reabsorption of calcium (i.e., renal leak hypercalciuria) and effects that increase bone resorption of calcium (i.e., resorptive hypercalciuria).
f. Hypercalcemia occurs in approximately one third of cats with calcium oxalate stones, and idiopathic hypercalcemia in cats has become increasingly common in the past 15 years. Many cats with idiopathic hypercalcemia also have calcium oxalate stones. Affected cats often have a history of having been fed acidifying diets, and chronic subclinical acidosis may play a role in development of hypercalcemia, hypercalciuria, and calcium oxalate urolithiasis. High fiber diets and prednisone therapy have been used to manage cats with idiopathic hypercalcemia, but it is not yet clear if this approach decreases occurrence of urolithiasis.
10. Citrate forms a soluble complex with calcium and normally may be an inhibitor of calcium oxalate formation. Acidosis may be associated with decreased urinary citrate excretion and, thus, may predispose to calcium oxalate stone formation.
11. The role of diet in oxalate urolithiasis in dogs and cats is unclear. The following conclusions are based on recent studies of diet composition and risk of calcium oxalate urolithiasis:
a. One predictor of stone mineral crystallization and growth is the degree of urine supersaturation with the crystalloid in question. Relative supersaturation (RSS) is the ratio of the activity product to the solubility product for stone-forming salts such as calcium oxalate and magnesium ammonium phosphate. RSS values of greater than 1 indicate supersaturation and values of less than 1 indicate undersaturation. Computer programs have been developed to determine RSS using urine pH and the concentrations of various inorganic and organic urinary electrolytes (Robertson WG, et al: 2002).
b. Higher RSS of urine with calcium oxalate has been observed in dogs with a history of forming calcium oxalate stones as compared with non–stone-forming dogs of similar age, breed, and sex (Stevenson AE, et al: 2003).
c. In dogs, canned food diets with the highest amounts of protein, fat, calcium, phosphorus, magnesium, sodium, potassium, chloride, or moisture were associated with decreased risk of calcium oxalate urolithiasis. Canned food diets with the highest amount of carbohydrate were associated with increased risk of calcium oxalate urolithiasis (Lekcharoensuk C, et al: 2002).
d. In cats, diets low in sodium or potassium or formulated to maximize urine acidity and those with moderate fat or carbohydrate content were associated with increased risk of calcium oxalate urolithiasis. Diets with high moisture or protein content and with moderate magnesium, phosphorus, or calcium contents were associated with decreased risk of calcium oxalate urolithiasis (Lekcharoensuk C, et al: 2001). Widespread use of acidifying diets in cats may play a role in development of urolithiasis in this species.
e. RSS of urine with calcium oxalate was compared in normal miniature Schnauzers and Labrador retrievers fed a 7% moisture diet with 0.06 g sodium/100 kcal as compared to the same diet supplemented with water (73% moisture) or sodium (0.2 to 0.3 g sodium/100 kcal). Increased moisture decreased calcium oxalate RSS in the miniature Schnauzers but not in the Labrador retrievers. Increased sodium content decreased calcium oxalate RSS in both breeds (Stevenson AE, et al: 2003). This study contradicts previous concerns that diets with large amounts of sodium may facilitate calciuresis and predispose to calcium oxalate urolithiasis.
f. In dogs, dry food diets with the lowest concentrations of sodium, phosphorus, calcium, chloride, protein, magnesium, or potassium were associated with increased risk of calcium oxalate urolithiasis. Diets with high urinary acidifying potential and low moisture content also were associated with increased risk of calcium oxalate urolithiasis (Lekcharoensuk C, et al: 2002).
g. In a comparison of nutrient intake and urine composition in calcium oxalate stone-forming dogs as compared with healthy control dogs, stone-forming dogs had lower intakes of sodium, calcium, potassium, and phosphorus and higher urinary calcium and oxalate concentrations, calcium excretion, and calcium oxalate RSS. Feeding Royal Canin’s Urinary SO Diet for 1 month resulted in increased intake of moisture, sodium, and fat and decreased intake of potassium and calcium and decreased urinary concentrations of calcium and oxalate, calcium excretion, and calcium oxalate RSS (Stevenson AE, et al: 2004).
h. Although it may seem paradoxical that a low calcium diet would be associated with a higher risk of calcium oxalate urolithiasis, this increased risk presumably occurs because diets restricted in calcium but not oxalate can result in decreased formation of insoluble, poorly absorbed calcium oxalate complexes in the gastrointestinal tract. As a consequence, more oxalate is absorbed, leading to hyperoxaluria, which is a bigger risk factor for calcium oxalate urolithiasis than hypercalciuria alone.
i. Healthy beagle dogs were fed a canned diet designed to decrease calcium oxalate urolith recurrence (Hill’s Prescription Diet u/d) with and without NaCl supplementation (1.2% versus 0.24% sodium on a dry matter basis). On the sodium-supplemented diet, 24-hour urine volume and calcium excretion increased, but there was no change in urine calcium concentration. Urine oxalate concentration and calcium oxalate RSS were lower on the NaCl supplemented diet. Hence, propensity to calcium oxalate crystallization was decreased on the NaCl-supplemented diet despite an increase in 24-hour urinary excretion of calcium (Lulich JP, et al: 2005).

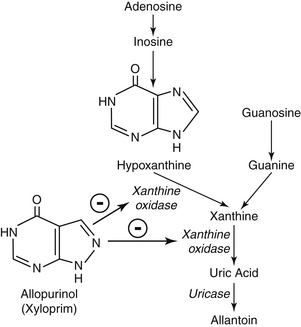
Urate Urolithiasis
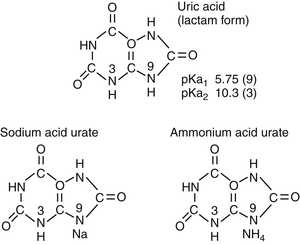
1. Urate stones in dogs usually are composed of the monobasic ammonium salt of uric acid (ammonium acid urate) (Figure 9-9). In human beings, they usually are composed of uric acid. Urate stones found in dogs with portosystemic shunts often contain struvite in addition to urate.
2. Urate stones are found most often in the Dalmatian and English bulldog. Other breeds also may be affected (e.g., miniature Schnauzer, Yorkshire terrier, Shih tzu). Urate stones may be found in dogs with portosystemic shunts, possibly due to reduced conversion of ammonia to urea and uric acid to allantoin. Urate stones generally occur uncommonly in cats.
3. Males are clinically affected much more commonly than females (especially in Dalmatians) possibly because the small stones become lodged in the urethra of males, leading to signs of urinary tract obstruction. Dalmatian dogs may be asymptomatic for their urate stones until an episode of obstruction occurs or the stones become quite large.
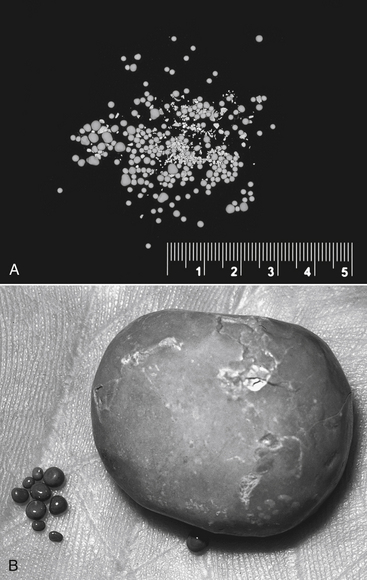
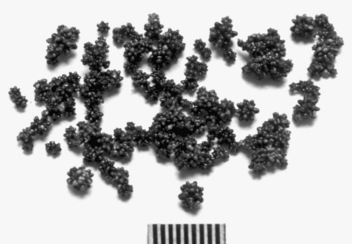
4. Urate calculi are small, brittle, spherical stones with concentric lamination. They usually are multiple in number and light yellow, brown, or green in color. (see Figure 9-10.)
8. A defect in uric acid metabolism in the Dalmatian dog is a predisposing factor for urate urolithiasis. This defect is a predisposing factor and not a primary cause of urolithiasis because Dalmatian dogs that do not develop stones also excrete large amounts of urate in their urine and other breeds (e.g., English bulldog) also may develop urate urolithiasis.
b. In dogs other than Dalmatians, uric acid is converted to allantoin in the liver by the enzyme uricase.
c. Dalmatian dogs have higher plasma uric acid concentrations and excrete much more uric acid in their urine than do other dogs.
d. The defect in uric acid metabolism in the Dalmatian is not caused by absence of hepatic uricase. The enzyme is present in the liver of Dalmatians in amounts comparable with those found in other breeds. Impaired transport of uric acid into hepatocytes may reduce the rate of hepatic oxidation in Dalmatians.
Cystine Urolithiasis
2. Cystine stones have been reported in many breeds of dog including English bulldogs, Newfoundlands, dachshunds, Irish terriers, Basset hounds, and bullmastiffs.
3. In most studies, cystine stones are found almost exclusively in male dogs. However, both male and female Newfoundlands are affected.
5. Canine cystinuria is an inherited disorder of renal tubular transport involving cystine or cystine plus other amino acids (often ornithine, lysine, and arginine). Not all dogs with cystinuria develop urolithiasis. Therefore, cystinuria is considered to be a predisposing rather than a primary causative factor.
6. Cystinuria is inherited as an autosomal recessive trait in the Newfoundland and is associated with a mutation in the SLC3A1 amino acid transporter gene. Where tested in other breeds of dog with cystinuria, the SLC3A1 gene was not involved, supporting the suspicion that cystinuria is genetically heterogenous in dogs as it is in humans.
8. Cystine stones are composed entirely of cystine. Qualitative kits for stone analysis may give false positive reactions for cystine, which may have falsely increased the frequency of cystine stones in early surveys. Hence, quantitative analysis of stones is necessary.
12. When it occurs, UTI usually is a complication of cystine urolithiasis rather than a predisposing cause.
Silicate Urolithiasis
2. These stones are composed primarily of silica (as silicon dioxide) but small amounts of other minerals such as struvite also may be present. Qualitative stone analysis kits do not detect silica, and quantitative analysis is necessary.
3. In dogs, silicate stones are gray-white or brownish and usually multiple in number. They frequently have a jack-like appearance. (see Figure 9-12.) Not all silica stones have this jack-like appearance, however, and not all jack-stones are silicates. Urate and struvite stones also may have a jack-like appearance.
6. The role of diet in spontaneously occurring silicate urolithiasis of dogs has not been determined, but diets high in corn gluten or soybean hulls are suspected to be contributory. An experimental atherogenic diet containing 12% silicic acid and 3% magnesium silicate resulted in silicate urolithiasis involving the kidneys, bladder, and urethra of dogs after as short a time as 4 months on the diet.
7. UTI, when it occurs, appears to be a complication of rather than a predisposing factor to silicate urolithiasis.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


