U
Upper Gastrointestinal Radiographic Contrast Series
OVERVIEW AND GOALS
• To identify abnormalities of the stomach and/or small intestinal tract. Morphologic and/or functional abnormalities may be identified.
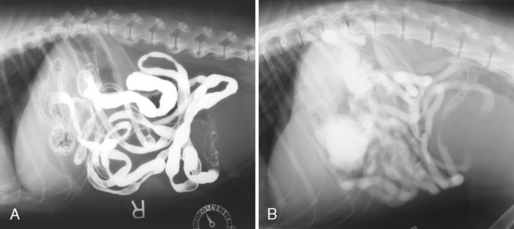
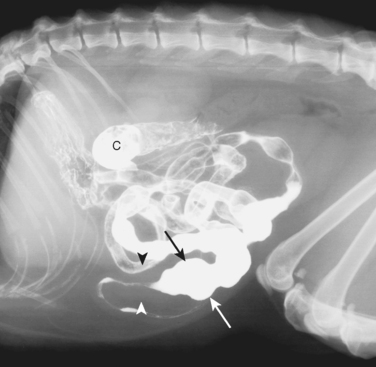
• The upper gastrointestinal (UGI) radiographic contrast series is most commonly performed using barium, which gives the best mucosal detail and therefore the best evaluation of morphology. The study may be performed with an iodinated contrast agent; these do not give good mucosal detail and are most useful for evaluating gastrointestinal (GI) integrity and patency.
CONTRAINDICATIONS
EQUIPMENT, ANESTHESIA
• Drugs for restraint (used only if absolutely necessary). The following agents have been shown to have the least effect on motility and should be used if a motility disorder is suspected. The effect on gastrointestinal motility of other newer sedative drugs has not been proven, so these agents cannot be recommended:
○ Cats: midazolam, 0.44 mg/kg; ketamine, 13.2 mg/kg:
▪ These drugs are given in separate syringes IM approximately 20 minutes prior to the procedure. If a motility abnormality is not of concern (i.e., determining if obstruction is present), the following combination is recommended for cats; this will give better and more consistent restraint than the midazolam/ketamine combination. The following drugs are also given IM approximately 20 minutes prior to the procedure and should be avoided if animal is elderly or systemically ill:
ANTICIPATED TIME
• About 6 hours to complete the study (barium); actual time spent performing the study is approximately 1.5 hours.
• About 2-3 hours to complete the study (iodinated contrast agents); actual time spent performing the study is approximately 1 hour.
POSSIBLE COMPLICATIONS AND COMMON ERRORS TO AVOID
• Vomiting and aspiration of barium: if the animal has projectile vomiting and/or radiographic evidence of severe gastric fluid retention, the risks involved in performing the UGI radiographic contrast series may outweigh the potential benefits.
• Aspiration of iodinated contrast agents: ionic iodinated contrast agents can cause severe (and fatal) pulmonary edema if aspirated. These agents should be administered only via orogastric intubation.
• Administration of too low a volume of barium:
○ This is the most common technical error in this study (occurs more often than administration of the proper volume of barium)
PROCEDURE
• Administer contrast:
○ Barium dosage: 10 mL/kg PO. If too low a volume of barium is used, artifactual delayed gastric emptying can occur and distension of the intestinal segments will not be achieved. Administration via orogastric tube is preferred, but barium may be administered per os; or
○ Iodinated contrast agent: Gastrografin/Renografin, 2-7 mL/kg PO, with total dose not to exceed 50 mL; or iohexol, 10 mL/kg PO of diluted iohexol (240-875 mg I/mL diluted 1:1 to 1:3). Administration via orogastric tube is necessary with the use of ionic iodinated agents (to avoid aspiration); administration via orogastric tube is preferred with the use of nonionic iodinated contrast agents.
• Obtain films:
○ Film sequence and views for barium. This sequence is a routine timetable. The timing of films can be altered as the study progresses, based on what is found in the study:
▪ Immediate: right and left lateral, ventrodorsal and dorsoventral
□ The dorsoventral view provides better evaluation of the body and pyloric region of the stomach and it is important to obtain this view in the immediate film series. However, it can be difficult to position the patient for a dorsoventral view, and ventrodorsal views are preferred for the remainder of the film series.
○ Film sequence and views for iodinated contrast agents. This sequence is a routine timetable. The timing of films can be altered as the study progresses, based on what is found in the study:
▪ Immediate: right and left lateral, ventrodorsal and dorsoventral:
□ The dorsoventral view provides better evaluation of the body and pyloric region of the stomach, and it is important to obtain this view in the immediate film series. However, it can be difficult to position the patient for a dorsoventral view, and ventrodorsal views are preferred for the remainder of the film series.
• By definition, the UGI radiographic contrast series is considered to be complete when contrast has both emptied from the stomach and has entered the large intestine.
• Films may be taken beyond this point if an abnormality has been noted during the examination. For example, in an animal with retention of barium in the stomach, the UGI radiographic contrast series should be continued until the stomach empties or an abnormality to account for the barium retention is noted.
POSTPROCEDURE
• There are no postprocedure considerations for a routine UGI radiographic contrast series other than informing the client that stools may have a paler color for several defecations after the procedure.
ALTERNATIVES AND THEIR RELATIVE MERITS
• Endoscopy:
○ Endoscopy allows visualization of the mucosal surface of the stomach and duodenum and allows tissue biopsies to be performed.
• Abdominal ultrasonography:
○ However, ultrasonographic evaluation of the GI tract can be severely limited by gas in the tract. Interpretation of ultrasound images of the GI tract requires an experienced sonographer, and many GI disease processes do not cause significant changes in the ultrasonographic appearance of the intestine.
• Exploratory laparotomy:
○ Allows assessment of the entire length of the GI tract and full-thickness gastric and intestinal biopsies. However, general anesthesia, invasiveness, and recovery/incision healing time make laparotomy a second-order diagnostic modality after lesser invasive evaluations such as plain radiography, UGI radiographic contrast series, ultrasonography, and/or endoscopy.



