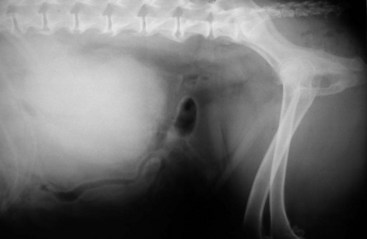
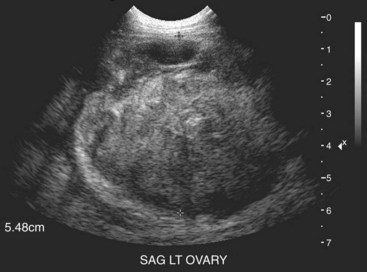
26 Ovarian tumors are uncommon in dogs and cats, resulting in part from the routine practice of ovariohysterectomy (OHE) in many areas of the world. The overall reported prevalence in dogs is 0.5% to 1.2%,1–3 with an estimated prevalence of 6.25% in intact bitches.4 Ovarian tumors are equally rare in cats, with a reported prevalence of 0.7% to 3.6% in intact queens.5,6 These numbers are primarily derived from pathology surveys and likely overestimate the true incidence in the pet population. Breed predilections are also difficult to discern; however, German shepherd dogs, Boxers, Yorkshire terriers, poodles, and Boston terriers appear to be most commonly affected.2,7,8 Aside from germ cell tumors and specifically teratomas, most ovarian tumors develop in older dogs (approximately 6 years of age and older).2,7–9 Teratomas are often found in younger dogs (≤6 years of age).7,8,10,11 Ovarian tumors have been reported in cats ranging from less than 1 year to 20 years (mean age: 6.7 years).12–15 Due to the complexity of the canine ovary, a variety of histologic tumor types may occur. Historically, canine ovarian tumors have been classified based on the World Health Organization (WHO) classification scheme for human ovarian tumors, with primary tumor types including epithelial tumors, germ cell tumors, sex cord stromal (gonadostromal) tumors, and mesenchymal tumors.2,8,16,17 Recently, the human WHO classification system was revised to subdivide each of the aforementioned categories into histologic types based on morphologic similarities; the use of immunohistochemistry has aided in further differentiating ovarian tumors.18 Attempts to recapitulate such classification schemes in dogs have been reported but are not routinely employed.19,20 Epithelial tumors arise from the outer surface of the ovary9 and according to several reports are most common.2,8,16 Malignant tumors outnumber benign tumors,7,8,16 and larger size is suggestive of malignancy.8,16 Malignant histologies include papillary adenocarcinomas, tubular adenocarcinomas, and undifferentiated carcinomas; benign tumors such as rete adenomas, papillary adenomas and cystadenomas also occur.2,8,16 Reportedly, 48% of adenocarcinomas will metastasize, generally within the peritoneal cavity to the intraabdominal lymph nodes, omentum, and liver.8 Direct tumor cell implantation and subsequent malignant effusion may also occur.3,8 Although most are unilateral, bilateral epithelial ovarian tumors have been described.8 Cysts in the contralateral ovary, as well as cystic endometrial hyperplasia, may also be found. Epithelial ovarian tumors routinely express cytokeratin AE1/AE3 (CK AE1/AE3), vimentin, and desmin.19,20 Although papillary adenocarcinomas also demonstrate placental alkaline phosphatase (PLAP) and cytokeratin 7 (CK 7) immunoreactivity, positive immunoreactivity appears to be less frequent in tubular adenocarcinomas.19 Alpha fetoprotein (AFP),19 S100,19 and endothelin-A (ET-A)21 are variably expressed. Faint to strong intracytoplasmic cyclooxygenase-2 (COX-2)22 and endothelin-1 (ET-1)21 immunoreactivity has been reported in 81% and 83% of canine ovarian carcinomas, respectively. Inhibin-α (INH-α), a glycopeptide synthesized in gonadal cells of the ovaries, inhibits pituitary secretion of follicle-stimulating hormone (FSH), and it has been described as a sensitive and specific marker for granulosa-theca cell tumor (GTCT).23 Therefore epithelial tumor cells should not express INH-α, and demonstration of INH-α expression has resulted in reclassification of epithelial tumors as GTCT.20 Sex cord stromal tumors, specifically GTCT, are also common and likely second in occurrence to epithelial tumors. Less common histologies include Sertoli-Leydig tumors, thecomas, and luteomas. These tumors arise from the specialized estrogen- and progesterone-producing gonadal stroma of the ovary and therefore have the potential to secrete these steroid hormones if functional.3,4,8,16 The metastatic rate of GTCT is low, occurring in approximately 20% of cases.3,8,9,16 Metastatic sites include sublumbar lymph nodes, pancreas, and lungs, with peritoneal carcinomatosis noted in some cases.1,3,8,16 Although rare, thecomas and luteomas are for the most part considered benign.8,16 Although most sex cord stromal tumors are unilateral, bilateral tumors are possible, especially among Sertoli-Leydig tumors.8 Concomitant cystic endometrial hyperplasia and cysts in the contralateral ovary appear common within this group.8 Solid, nest, cord, palisade, cystic, and spindle are the histologic patterns described for GTCT, and a mixture of these may exist within a single tumor.8,19 GTCTs are generally vimentin,19 S100,19 and INH-α20 positive, although one study has reported INH-α negative GTCT.19 Variable expression of CK AE1/AE3,20 CK 7,20 and ET-A21 has been described, and moderate-to-strong intracytoplasmic ET-1 immunoreactivity has been detected in 88% of canine GTCT. Germ cell tumors, including dysgerminomas, teratomas, and malignant teratomas (teratocarcinomas), arise from primordial germ cells of the ovary.8,16,24 Concurrent cysts in the contralateral ovary and uterine abnormalities such as pyometra and cystic endometrial hyperplasia are common.24 Dysgerminomas, also known as ovarian seminomas, are most common in this group and arise from undifferentiated germ cells. Histologically, these tumors consist of a uniform population of cells resembling ovarian primordial germ cells.3,8,16 Bilateral dysgerminomas have been reported; however, most are unilateral.8,16,24 The reported metastatic rate is low (10% to 30%), with sites of metastasis including lymph nodes, liver, kidney, omentum, pancreas, and adrenal glands.3,8,9,24–26 Teratomas are composed of germ cells that undergo differentiation into at least two germinal cell layers and any combination of tissues can be seen. These tissues are usually well differentiated, and tissues from virtually any organ (excluding ovary or testis) may be present. Malignant teratomas are composed of predominantly immature, undifferentiated tissues resembling those of the embryo.24 Metastasis has been noted in up to 50%. Although distant visceral metastasis can occur, peritoneal metastasis with carcinomatosis is most common.8,9,24 Germ cell tumors, specifically dysgerminomas, are vimentin positive and PLAP, CK 7, desmin, S100, CK AE1/AE3, and INH-α negative.19 Mesenchymal ovarian tumors are rare. Reported tumor types include hemangiosarcoma,2,16 hemangioma,16 and leiomyoma.2,16 Behavior of this group is difficult to predict because information in the literature is sparse. In addition to the various primary ovarian tumors, other differential diagnoses should be considered. These include ovarian cysts, paraovarian cysts, cystic rete tubules, vascular hamartomas, and adenomatous hyperplasia of the rete ovarii. Although rare, metastasis to the ovary has been reported in cases of mammary (especially inflammatory carcinoma),27 intestinal, and pancreatic carcinoma, as well as lymphoma.16 Reported feline ovarian tumor classifications include epithelial, germ cell, and sex cord stromal tumors. Although mesenchymal ovarian tumors have not been reported in cats, it seems plausible that they may occur. Ovarian involvement in cats with lymphoma has been documented.15 Sex cord stromal tumors are most common in cats, accounting for at least half of reported cases. They are often unilateral. Of these, GTCTs are most common and approximately 50% are malignant. Metastatic sites include the peritoneum, regional lymph nodes, omentum, diaphragm, kidney, spleen, liver, and lungs.15 Luteomas, thecomas, and Sertoli-Leydig cell tumors are rare and typically benign. Germ cell tumors are also rare in cats. Of these, dysgerminomas are most common.15 They are generally considered benign, yet metastasis has been reported in 20% to 33% of cases.15 Teratomas have been rarely documented.15,28 Epithelial tumors are perhaps the least common ovarian tumor in the cat. Cystadenomas and adenocarcinomas have been described. Metastasis to the lungs, liver, and abdominal peritoneum was seen in one case of ovarian adenocarcinoma.15 History and clinical signs associated with canine ovarian tumors vary, depending on the tissue of origin. Although initially insidious, ovarian tumors grow to the point of being palpable and clinical signs are typically referable to a space-occupying abdominal mass (Figure 26-1).9,29–31 Functional sex cord stromal tumors may produce one or multiple hormones, or they may be nonfunctional.8,16,32 Sex cord stromal tumors that produce steroid hormones such as estrogen may cause vulvar enlargement, sanguineous vulvar discharge, persistent estrus, alopecia, and aplastic pancytopenia, whereas excessive progesterone production may cause cystic endometrial hyperplasia and pyometra.3,8,9,16,30 Hyperadrenocorticism was reported in a dog with an ovarian-steroid tumor resembling a luteoma, and the associated clinical signs resolved following OHE.33 Germ cell tumors have been associated with evidence of hormonal dysfunction, although they are most often associated with clinical signs referable to a space-occupying abdominal mass.24 Ovarian tumors in cats also have an insidious onset and eventually grow to the point of being detectable by abdominal palpation. Signs referable to a space-occupying abdominal mass such as weight loss, lethargy, vomiting, ascites, and abdominal distension are often noted. GTCTs are most common, and they are generally functional, producing estrogen, progesterone, or testosterone. Clinical signs of hyperestrogenism, including persistent estrus, alopecia, and endometrial hyperplasia, have been reported.15 Virilizing behavior secondary to a testosterone-producing thecoma of the ovarian stump was reported in a 6-year-old domestic shorthair cat.34 Laboratory abnormalities attributable to ovarian tumors are generally not noted. However, hypercalcemia secondary to tumor production of parathyroid hormone–related peptide (PTH-rP) has been reported in a dog with ovarian adenocarcinoma.31 Thoracic radiographs should be evaluated for evidence of metastatic disease. Abdominal imaging, specifically ultrasound, is useful in identifying ovarian masses and associated abdominal metastasis or uterine abnormalities (Figure 26-2). Ultrasonographic patterns include solid, solid with cystic component, and cystic. Malignant tumors are typically solid, whereas benign tumors are generally cystic with smooth borders. Concurrent uterine abnormalities such as pyometra and cystic endometrial hyperplasia may be detectable via ultrasound in up to 50% of dogs.35 Because the risk of tumor seeding is high, transabdominal needle biopsies of ovarian tumors are not recommended. If present, abdominal fluid may be safely collected, and cytologic evaluation of fluid often is suggestive of malignant effusions. In a series of 19 cases with a variety of ovarian tumors, cytologic diagnosis was consistent with histopathology in 94.7% (Figure 26-3).2 Finally, if a functional tumor is suspected, evaluation of vaginal cytology for evidence of estrogen-induced cornification is also indicated.
Tumors of the Female Reproductive System
Ovarian Tumors
Pathology and Natural Behavior
Epithelial Tumors
Sex Cord Stomal Tumors
Germ Cell Tumors
Mesenchymal Tumors
Miscellaneous
Feline Ovarian Tumors
History and Clinical Signs
Feline Ovarian Tumors
Diagnostic Techniques and Work-Up
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Tumors of the Female Reproductive System