Chapter 16 Treatment of Cardiac Arrhythmias and Conduction Disturbances
INTRODUCTION TO TREATMENT OF CARDIAC ARRHYTHMIAS
General Remarks
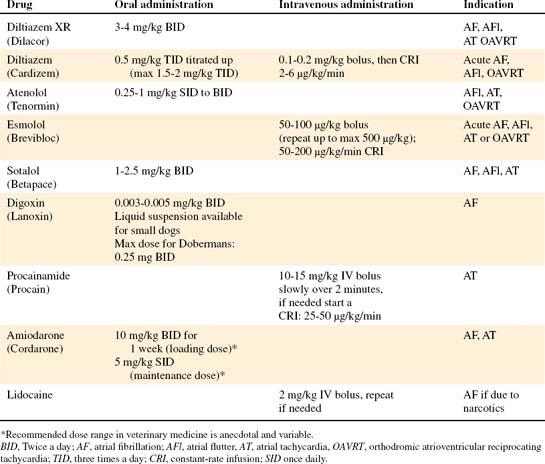
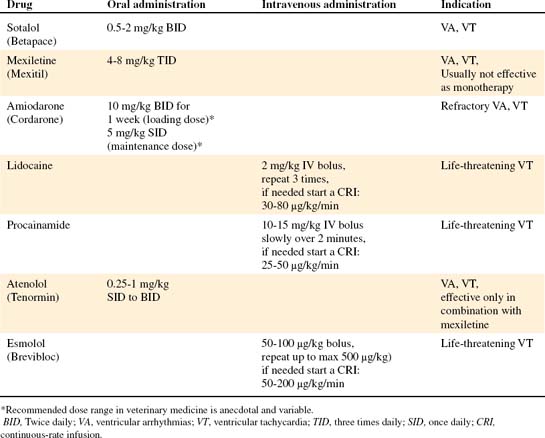
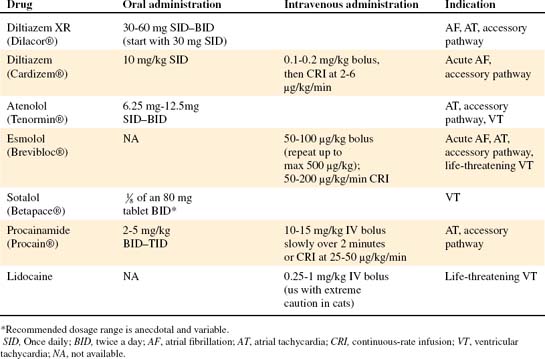
The decision regarding how and when to treat an arrhythmia should be based on the clinical signs and urgency of intervention. Emergency management using intravenous drugs may be required before a 24-hour Holter recording can be obtained. Both diltiazem and esmolol are available in an IV formulation, allowing emergency treatment of excessively rapid supraventricular arrhythmias (SVAs), Lidocaine is the most important intravenous drug used for life-threatening ventricular arrhythmias.
ATRIAL FIBRILLATION
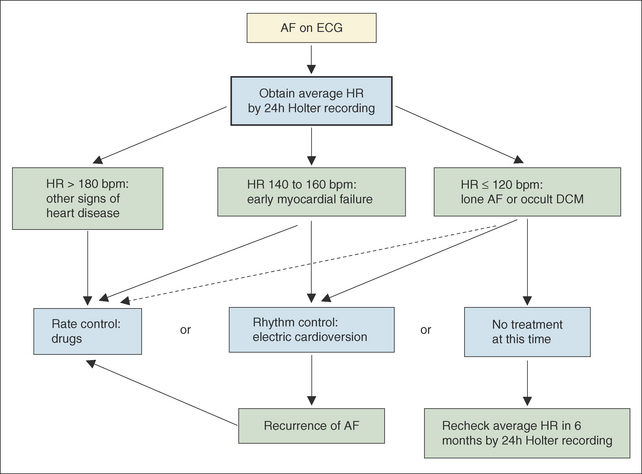
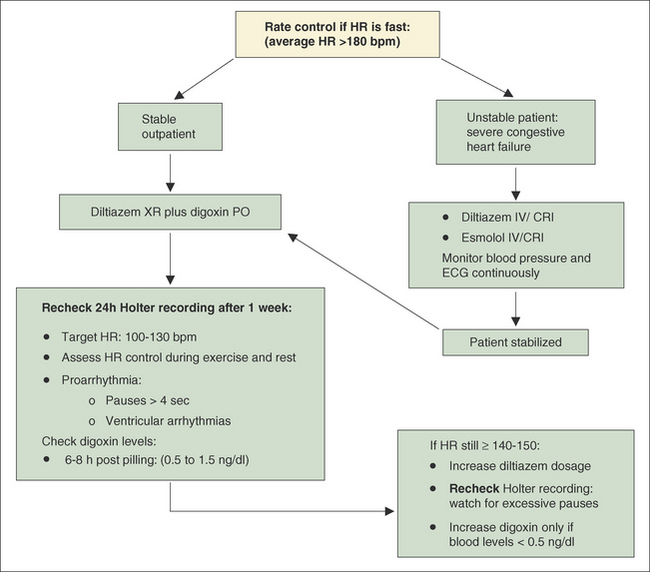
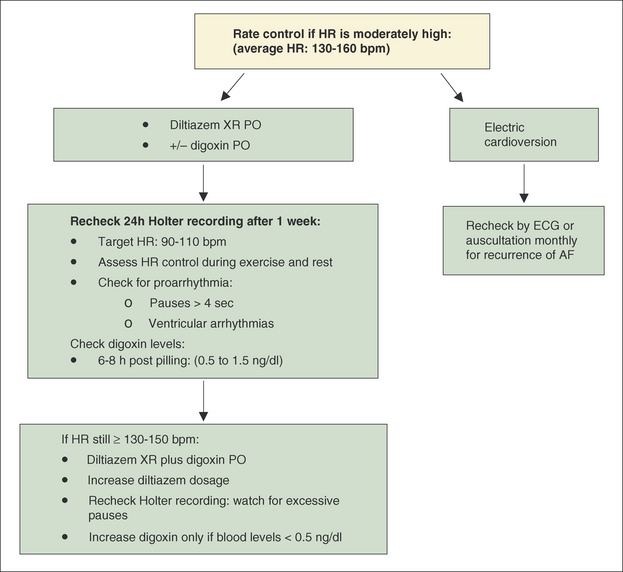
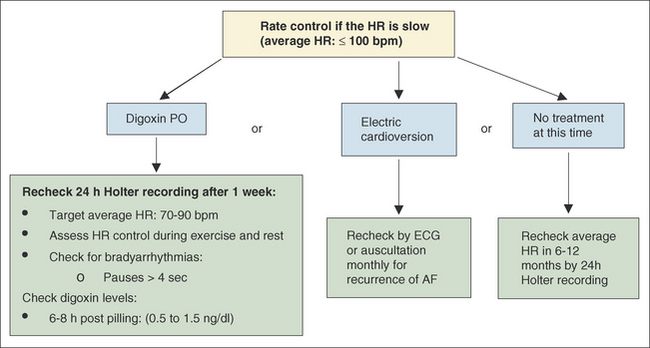
Figure 16-1 Flow chart describing the approach to treatment of atrial fibrillation (AF) based on the average heart rate (HR) of a patient as determined by a 24-hour Holter recording. AF, Atrial fibrillation; HR, heart rate; bpm, beats per minute; DCM, dilated cardiomyopathy.