Chapter 16
Transtracheal and Bronchoalveolar Washes
Respiratory flushes or washes sample the contents of the airways, the trachea, bronchi, and alveolar spaces. These samples frequently provide clinically useful information of the pulmonary disease process and may also provide definitive diagnosis in some patients. Pulmonary disease is often defined by the area that it affects (e.g., bronchitis) or by the changes that may occur as a result of the disease process (e.g., bronchiectasis); however, the underlying pathology may be variable with these disease presentations, and cytology and culture of a lower respiratory tract sample may be helpful in determining the etiology. In pathologies that solely involve abnormal structure or function of the airways or in diseases that do not have direct airway involvement, which may include some primary or metastatic neoplasms, the information obtained from a flush or wash sample may be limited.1,2 Cytology of flush or wash samples may, however, be highly sensitive in cases of inflammatory airway disease.3
Tracheal wash or bronchoalveolar lavage (TW/BAL) samples are quick, easy, and inexpensive ways to obtain diagnostic samples from the respiratory tree. Although complications are rare, subcutaneous emphysema, pneumomediastinum, hemorrhage, resultant hypoxia, needle tract infection, transient hemoptysis, bronchoconstriction, and other complications have been reported.4–7
It is frequently helpful to perform radiography in conjunction with the wash procedure, although radiographic changes may not always be apparent in the early stages of respiratory disease.8,9 Radiography prior to a flush or wash procedure may be invaluable if the disease is focal because this will indicate which lung lobe is most likely to provide a diagnostic yield and allow selective sampling, particularly if bronchoscope-guided lavage is used. If the disease is diffuse, sampling of any area of the lung may be representative, although sampling from multiple sites is more likely to provide a diagnostic yield.10
The cell types noted in the sample may vary, depending on the site of sampling (Table 16-1 and Table 16-2).
TABLE 16-1
Lining Cells of the Lower Respiratory Tract That May Be Noted on Tracheal Wash or Bronchoalveolar Lavage Sampling
| Airway | Lining cell |
| Large airway, trachea, and bronchi | Ciliated columnar epithelium, goblet cell |
| Bronchiole | Columnar to cuboidal epithelium, ciliated to nonciliated |
| Alveolus | Type I pneumocyte (not commonly observed on bronchoalveolar lavage cytology) |
From Bacha WJ Jr., Bacha LM: Respiratory system. Anderson RC: Nematode Parasites of Vertebrates. Their Development and Transmission. 2nd Edition. CABI Publishing, Wallingford, Oxon (UK) 2000.
TABLE 16-2
Average of Mean Percentage Cell Differential of Nonepithelial Populations from a Number of Studies of Bronchoalveolar Lavage Samples from Healthy Dogs and Cats

Technique of Tracheal Wash and Bronchoalveolar Lavage
Many reviews of the sampling techniques exist.11–14 However, a brief summary is outlined here.
Transtracheal Sampling
• The skin over the cranioventral larynx is clipped and the site is prepared as for aseptic surgery. Surgical gloves should be worn.
• A small amount of 1% to 2% lidocaine is injected into subcutaneous tissue. Very light sedation may be helpful in cats and small dogs;4 intravenous ketamine has been recommended for sedation of cats.5
• The animal is restrained in a sitting position or in sternal recumbency, with the neck extended. Overextension of the neck, however, may result in increased oropharyngeal contamination.
• A small, triangular depression is digitally palpated just cranial to the ridge of the cricoid cartilage. This is the location of the cricothyroid ligament and of needle insertion (Figure 16-1). Alternatively, the catheter may be inserted between two tracheal rings 1 to 3 cm below the larynx (e.g., C2 to C3, or C3 to C4).15
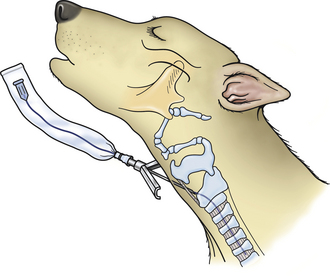
Figure 16-1 Diagrammatic representation of needle placement through the cricothyroid ligament of the larynx.
• Using a large commercial intravenous catheter set, “through the needle,” or intravascular catheter and a 3.5-French (Fr) polyethylene urinary catheter, with the needle directed slightly caudad, the skin, subcutaneous tissue, and cricothyroid ligament of the larynx, or ligament between the tracheal rings, are penetrated.5 Smaller catheters are recommended for cats and very small dogs.
• Once in the tracheal lumen, the needle is positioned parallel to the trachea, and the catheter is advanced through the needle and down the lumen of the trachea to a level just above the carina. Insertion of the needle and passage of the catheter induces coughing in most animals.4,5
• The catheter should pass easily; if it does not, it may have become embedded in the dorsal tracheal wall or failed to enter the trachea and may be embedded in the peritracheal tissue.16 In either case, the needle and the entire catheter should be withdrawn and the procedure repeated. Also, the catheter may bend, causing it to advance toward the oropharynx, which results in the washing of the oropharynx, not the bronchial tree.
• Once the catheter is properly placed, the needle is withdrawn, leaving the catheter in place. With some severe pulmonary diseases, a sample may be obtained by simply aspirating after positioning the catheter. However, the infusion of saline into the bronchial tree is usually necessary before aspiration to obtain an adequate sample. A 12-mL (milliliter) or larger syringe containing 1 to 2 mL of nonbacteriostatic, sterile, buffered saline for every 5 kilogram (kg) of body weight is attached to the catheter. The saline is injected into the bronchial lumen until either the animal starts to cough or all of the fluid is injected.
• The animal will typically start coughing before all of the saline is injected, at which time aspiration must start. If coughing does not occur, coupage may be helpful. Only a small portion of the injected fluid will be retrieved. The injected fluid remaining in the tracheobronchial tree will be rapidly absorbed and is no cause for concern.4
• The operator aspirates for only a few seconds and then stops. Aspiration for a prolonged time results in more fluid being collected, but the chances of a contaminated wash are greatly increased because the animal will cough fluid into the oropharyngeal area and reaspirate the fluid, which now contains cellular and bacterial contaminants.
Maintaining gentle pressure on the puncture site for a few minutes generally inhibits the formation of subcutaneous emphysema.15 Applying mild pressure to the puncture site with a gauze wrap for 12 to 24 hours also helps eliminate the formation of subcutaneous emphysema.
Endotracheal Tube Technique
Alternatively, samples are collected through an endotracheal tube (Figure 16-2). This procedure requires general anesthesia. This technique may be used to obtain either a TW or a BAL. For a tracheal sample, the sample catheter extends beyond the end of the endotracheal tube but does not extend past the carina. The location of the carina is externally assessed as approximately the level of the fourth intercostal space.10 For a blind BAL, a sample tube of appropriate size for the patient (e.g., a 16-Fr polyvinyl chloride stomach tube in a medium- to large-sized dog, and a 5-Fr polypropylene urinary catheter in a cat) was shown to consistently maintain a snug fit between the external landmarks of the seventh and eleventh ribs, so the sample tubing should be a minimum length to reach the level of the eleventh rib.17,18 Sterile tubing should be used. Pretreatment with bronchodilators is recommended by some authors prior to BAL.7
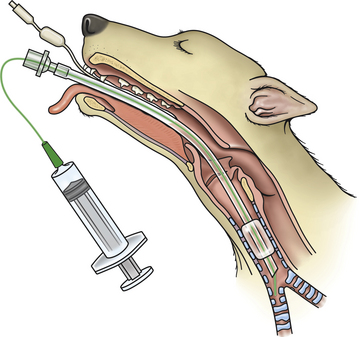
Figure 16-2 Diagrammatic representation of catheter placement and tracheal wash or bronchoalveolar lavage collection through an endotracheal tube.
• Once the patient has reached a suitable plane of anesthesia, an endotracheal tube should be carefully placed with as minimal contact with the oropharynx and larynx as may be achieved.
• Preoxygenation is recommended. Fitting of a T- or Y-piece to the endotracheal tube will allow delivery of oxygen and anesthetic gas throughout the procedure. If the leakage of gas is a particular concern to the veterinary staff, anesthesia may be maintained by injectable anesthetic agents administered via an intravenous (IV) catheter.
• The patient is placed in sternal or lateral recumbency; if the lateral position is used, it is preferable to place the most affected side down.14 In some cases, use of a foam wedge to elevate the cranial part of the thorax above that of the caudal part has been recommended.19
• A bronchoscope, tube, or catheter through which the sample will be obtained is introduced through the endotracheal tube, ensuring this does not contact the oropharynx.
The canine bronchial tree branches in an irregular manner and has been reviewed in detail.20 Briefly, when the patient is orientated in sternal recumbency, from the bronchial tree, the entrance to the right principal bronchus appears as almost a direct continuation of the trachea, with the left principal bronchus seen at a more acute angle. The first lobar bronchus on the right is the right cranial lung lobe, in the lateral wall of the bronchus opposite the carina. The next lobar bronchus is the right middle lung lobe, in the ventral floor, usually between the 6 and 8 o’clock positions. The right accessory lobe is located in the ventromedial to medial aspect of the right principal bronchus, just beyond the origin of the middle lobe bronchus, extending in a ventromedial direction. Beyond this bronchus is the lobar bronchus for the right caudal lung lobe. On the left the left cranial lung lobe is accessed ventrolateral to the lateral aspect of the left cranial bronchus. Beyond this, the left principal bronchus becomes the left caudal lung lobe bronchus. Figure 16-3 shows a cast of a canine bronchial tree to provide an idea of the branching that may be seen in vivo.
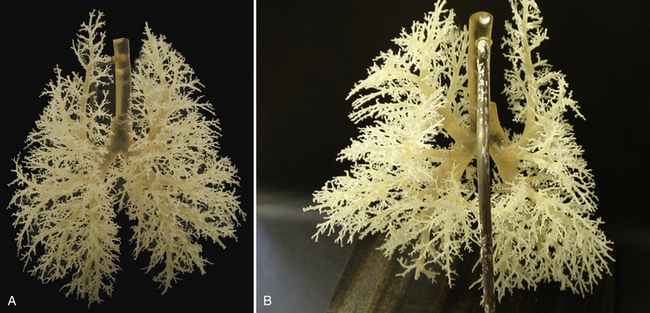
Figure 16-3 A, A cast of the canine bronchial tree. B, Close-up of the area of the bifurcation of the trachea to show the bronchial branching in more detail. (A, Courtesy of A. Crook, RVC, U.K.)
The feline bronchial tree has also been reviewed.21 The right principal bronchus is similarly a near continuation of the trachea, as in the dog, with the left principal bronchus at a slightly more acute angle. Entering the right principal bronchus, the right cranial bronchus is first encountered, arising lateral to the right principal bronchus and directly opposite the carina. Advancing caudally, the next lobar bronchus is the right middle lung lobe located ventrally. The right accessory lobe bronchus and the first segment of the right caudal lobar bronchus arise at approximately the same level, with the right accessory lobe bronchus being located ventromedially and the right caudal bronchus dorsally. The second segment of the right caudal lobe bronchus is more dorsal and located ventrally, with the third segment more caudal and dorsal. Entering the left principal bronchus, the left cranial lobar bronchus is lateral and slightly ventral. The continuation of the left principal bronchus enters the left caudal lobe bronchus, with the segmental bronchi branching alternately dorsally and ventrally as in the right caudal lobe. It may not be possible to enter all of the bronchi or even visualize the more caudal bronchi in all cats examined.
• If the patient is in lateral recumbency, the orientation and access to the lung for sampling may be altered.22
• When the desired level has been reached for a TW or a BAL (see previous), then fluid may be introduced. To optimize recovery of fluid from a BAL, the bronchoscope or tube should be wedged into the bronchi. This may be determined visually on a bronchoscope. If performing a blind BAL, then the tube should be advanced gently until it stops; it should then be withdrawn a few centimeters, rotated gently, and readvanced until resistance is felt at a consistent level.17
• Once a snug fit has been achieved, a syringe with an appropriate volume of fluid and an additional 5-mL of air to ensure complete delivery of the fluid is attached to the top of the sample tube. Volumes used may vary; however, a suitable volume in cats is reported to be aliquots of 5-mL/kg.23 This volume may be used in dogs, but volumes of 2-mL/kg have been reported to be adequate.24,25 Repeat aliquots may be administered until sufficient fluid is retrieved; however, no more than three aliquots are generally used.
• Fluid recovery may be affected by the tightness of the fit of the bronchoscope or sample tubing in the airway. In the double catheter technique, the catheter to collect the sample is placed a few centimeters above the level of the catheter delivering the fluid aliquot; the authors describing this technique have reported good fluid recovery without the need for a snug fit.26
Other measures that may increase fluid retrieval include tilting the head of the patient downward and rotating the patient with the lavaged lung area uppermost to encourage fluid drainage.27 This may be complicated in larger patients, and the risk of gastric dilation-volvulus in large, deep-chested dogs may also be a concern with rotation of these patients. Coupage may also be helpful.
Retrieved fluid should appear foamy if the sampling has been adequate and is reported to reflect the presence of surfactant.14
Other techniques that have been reported via bronchoscopic sampling are bronchial brushings and biopsy.15 One study suggested that in some instances, bronchial brushing may be a more sensitive test to assess for inflammation, although in one patient, BAL was the more sensitive test.28 However, the criteria to determine what constitutes inflammation from these types of samples alone is not clearly defined.
Bronchoscopy may also be used for treatment, as in the removal of tracheobronchial foreign bodies.29 Therapeutic bronchoalveolar lavage has also been described in one dog affected by pulmonary alveolar proteinosis.30
Sample Submission
Several studies in healthy patients have shown that no significant differences exist between different lobes of the lung lavaged either in overall cell numbers or differential counts.19,31 Therefore, increases of cells will be interpreted similarly, no matter which area of the lung the samples are derived from. The first aliquot is reported to have fewer epithelial cells and higher numbers of polymorphonuclear cells, and some authors recommend discarding the first aliquot, although it is unlikely to significantly affect clinical interpretation if the first aliquot is combined with subsequent aliquots.23
It is recommended to prepare fresh smears at the time of sample collection, within 30 minutes because cell morphology is not well preserved in TW/BAL samples.31 A direct smear of turbid fluid (or if mucous flecks are noted grossly), a smear of mucus material, and additional cytocentrifuged preparations are likely to provide the most information from the sample.
Recommendations for samples submitted to the laboratory are noted in Box 16-1. Guidelines for preparing smears from fluids are presented in Chapter 1.
If the TW/BAL is deemed unacceptable because of oropharyngeal contamination (or for any other reason) and is to be repeated, it should be repeated either immediately or after 48 hours. Even though a sterile saline solution is used for the wash, it induces a neutrophilic response that peaks about 24 hours after washing. If a TW/BAL is performed the next day (i.e., 24 hours after the first wash), an inflammatory response will be present, and it may be difficult to tell whether it is secondary to the prior wash or because of an inflammatory lung disease.32–34 However, no significant difference may exist in samples collected 48 hours apart.24,32,34 If a contaminated wash is obtained, it is ideal to wait at least 48 hours to collect a TW/BAL again because it allows the lungs time to clear the oropharyngeal contaminants. Sometimes, however, such a delay is not practical. Although some contaminants from the previous wash may be collected, if the TW/BAL is repeated immediately, the amount of oropharyngeal contamination should be minimal, and this may be preferable to waiting 48 hours.
Cell Counts
Cell counts are difficult to perform on TW/BAL fluids because of the mucous content, and the dilution factor may be variable.35 The method of obtaining cell counts is also varied in many studies of TW/BAL in dogs and cats, so values may not be directly comparable, and diagnostic significance is often difficult to determine.36 One study of cases of idiopathic pulmonary fibrosis found increased total cell counts in diseased individuals compared with controls, although differential cell counts were generally not altered.37 Cell counts are recommended by some authors to determine whether an adequate sample has been obtained and to assess whether resampling is necessary. However, this may not be easily applicable in the practice setting. Qualitative estimates (normal or increased) of cellularity may be done on stained sediment smears and may be useful.
Cytologic Evaluation
Mucus
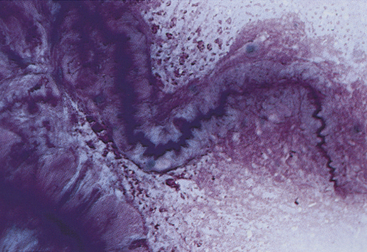
A small amount of mucus may be present in TW/BAL specimens from clinically normal dogs and cats. Mucus appears as amorphous sheets ranging from blue to pink or as homogeneous strands that are frequently twisted or whorled (Figure 16-4; see also Figures 16-7, 16-12, 16-13, 16-17, and 16-18).4,27 A granular appearance of the mucus is frequently associated with increased cellularity.4 Inflammation, irritation, or upper airway damage, which may be a result of chronic airway disease, may result in increased numbers of goblet cells, and an increased amount of mucus is generally present, possibly with altered mucus properties.4,32,38 In inflammatory conditions, mucus usually stains eosinophilic because of the incorporation of inflammatory proteins and material from lysed cells.4
Curschmann spirals (Figure 16-4) are mucous casts of small bronchioles that appear as spiral, twisted masses of mucus that may have perpendicular radiations, giving them a test tube-brush-like appearance.39 They may be seen in TW/BAL specimens from patients with any disorder that results in chronic, excessive production of mucus and are an indication of bronchiolar obstruction.
Cell Types
Many different types of cells (e.g., ciliated and nonciliated columnar cells, ciliated and nonciliated cuboidal cells, alveolar macrophages, neutrophils, eosinophils, lymphocytes, mast cells, erythrocytes, and dysplastic and neoplastic cells) may be seen in TW/BAL specimens (see Tables 16-1 and 16-2). Ciliated and nonciliated columnar and cuboidal cells and alveolar macrophages are the cell types seen in washings from normal dogs and cats. They are also seen in many disease states unless the washed area is filled with exudative secretions or the disease process has obliterated normal lung parenchyma. In one study in cats, storage of the bronchoalveolar lavage specimen for 24 hours or longer has been shown to result in decreased neutrophil percentages and increased eosinophil percentages. In a few individual cases, this change was sufficient to alter the cytologic interpretation.40 One study in dogs reported that neutrophil and eosinophil percentages were both decreased on the smears prepared at 24 hours after sampling compared with those prepared 3 hours after sampling.41 Cytocentrifugation has been reported to affect the cell populations, particularly reducing the number of small lymphocytes present.42 However, in one canine study, neutrophils were found to be more represented on cytospin preparations compared with direct smears of pelleted cells.43 One canine study suggested that age may influence differential cell counts, but the group size was small and the findings were at variance with a previous study, suggesting that further work may be needed to determine if age should be considered when assessing bronchoalveolar lavage cytology.44,45 When determining differential cell counts, it is difficult to be consistent when assessing the epithelial population, and many do not consider this essential to assess the sample. When assessing macrophages, neutrophils and eosinophils, counting 200 cells from a cytospin preparation, if available, has been shown to provide repeatable results.46
Columnar and Cuboidal Cells
Ciliated columnar cells (Figure 16-5 and Figure 16-6) have an elongated or cone shape, with cilia on their flattened apical ends. The nucleus, which is generally round to oval with a finely granular chromatin pattern, is present in the basal end of the cells, which often terminate in a thin tail.39 The ciliated cuboidal cells look similar to the ciliated columnar cells except that the cuboidal cells are as wide as they are tall. Nonciliated columnar and cuboidal cells look identical to their ciliated counterparts except for the absence of cilia. These cell types are normal findings in TW/BAL. If these cell types are predominant in a sample, the washing procedure probably sampled mainly bronchi and bronchioles (as opposed to alveolar spaces).
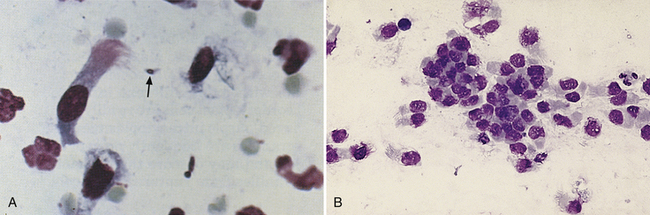
Figure 16-5 A, Tracheal wash or bronchoalveolar lavage from a dog with toxoplasmosis. A ciliated columnar cell, red blood cells, scattered neutrophils, and an extracellular Toxoplasma gondii organism (arrow) are shown. (Wright stain. Original magnification 250×.) B, Ciliated columnar cells are present both individually and in a cluster. The morphology of the cells in the cluster cannot be discerned. Cilia are evident on the cells that are well spread out. Many of the cells are traumatized as evidenced by their irregular nuclear outlines. (Wright stain. Original magnification 160×.)
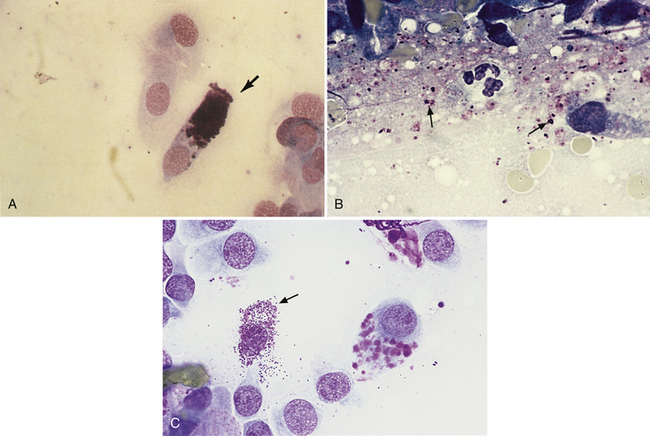
Figure 16-6 A, Tracheal wash or bronchoalveolar lavage from a dog. A goblet cell (arrow) and several ciliated columnar cells are present. (Wright stain, original magnification 250×). B, Granules from ruptured goblet cells are shown extracellularly (arrows) and must not be confused with bacterial cocci. (Wright stain. Original magnification 330×.) C, Goblet cells can be differentiated from mast cells (arrow), which have smaller granules.
Cuboidal and columnar epithelial cells may be present individually or in clusters (see Figure 16-5, B). Depending on the orientation of the cell on the slide (especially with cells in clusters), the cuboidal or columnar nature of the cells and cilia may be difficult to visualize. This is of little clinical significance, but these cells must not be interpreted as abnormal cell types.39 Also, the majority of the columnar cells may be poorly preserved in many washes (see Figure 16-5, B) as a result of the low protein fluid in which they are collected. Cells traumatized during slide preparation may show irregular nuclear outlines or be overtly ruptured (e.g., smudge cells).
Goblet Cells
Goblet cells (see Figure 16-6) are mucus-producing bronchial cells that are generally elongated (i.e., columnar) with a basally placed nucleus and round granules of mucin, which frequently distend the cytoplasm.39 Occasionally, the cytoplasm is so distended that the cell appears round. The granules stain from red to blue to clear with Romanowsky (e.g., Giemsa-Wright) stains. Free granules from ruptured goblet cells may be seen in the smear (see Figure 16-6, B). The shape of the cells and the large size of the granules are helpful in differentiating these cells from mast cells (see Figure 16-6, C). Goblet cells are not frequently seen; however, any chronic pulmonary irritant may result in increased numbers of goblet cells.
Macrophages
Alveolar macrophages (Figure 16-7) (see also Figures 16-9, 16-13, and 16-18) are readily found and are often the predominant cell type in TW/BAL samples from clinically normal animals. They are present in samples that have adequately washed the alveolar spaces and, therefore, are a useful indicator of sample adequacy. The nucleus is round to bean shaped and eccentrically positioned. A binucleate alveolar macrophage is rarely seen in clinically normal animals. Alveolar macrophages have abundant blue-gray granular cytoplasm. When they become activated, their cytoplasm becomes more abundant and vacuolated (i.e., foamy) and may contain phagocytized material (see Figure 16-7, B).31
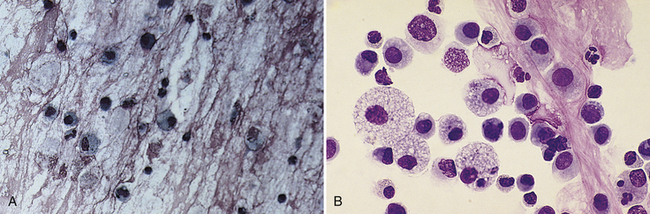
Figure 16-7 A, Tracheal wash or bronchoalveolar lavage (TW/BAL) from a dog. Many alveolar macrophages and some neutrophils are present in an eosinophilic mucous background. (Wright stain. Original magnification 132×.) B, TW/BAL from a dog. Numerous stimulated and unstimulated alveolar macrophages and scattered granulocytes and lymphocytes are present in strands of mucus. (Wright stain. Original magnification 250×.)
Eosinophils
Eosinophils (Figures 16-8, 16-9, and 16-10) are polymorphonuclear granulocytes that contain intracytoplasmic granules, many of which have an affinity for the acid dye, eosin (i.e., eosinophilic), which stains them red with Romanowsky stains.47 Increased numbers of eosinophils indicate a hypersensitivity reaction that is either allergic or parasitic;4 see the discussion on hypersensitivity later in this chapter.
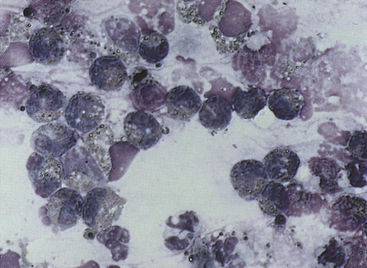
Figure 16-8 Tracheal wash or bronchoalveolar lavage from a dog.
Mucus, scattered neutrophils, and a large number of eosinophils are shown. Some extracellular bacterial rods, probably from oropharyngeal contamination, are also present. (Wright stain. Original magnification 330×.)
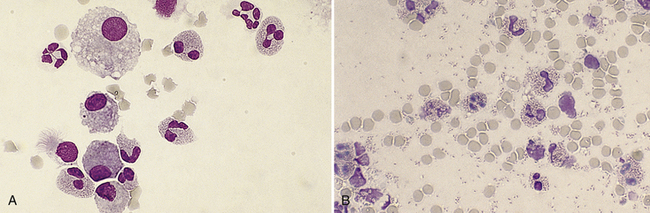
Figure 16-9 A, Tracheal wash or bronchoalveolar lavage specimen from a cat with a hypersensitivity reaction. Several eosinophils with bilobed and trilobed nuclei, scattered alveolar macrophages, two neutrophils with multilobulated nuclei, and a ciliated columnar epithelial cell are shown. The granules of the eosinophils are tightly packed, slender rods that may be easily overlooked. Note that the eosinophils are somewhat larger than the neutrophils and have less segmented nuclei. (Wright stain. Original magnification 250×.) B, Feline eosinophils. Granules are seen more easily in cells that are well spread out or partially ruptured. Many free eosinophil granules are seen in the background. (Wright stain. Original magnification 250×.)
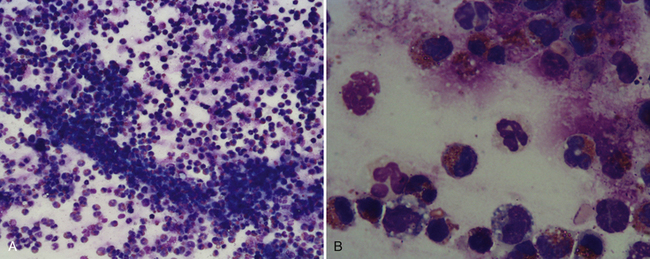
Figure 16-10 Bronchoalveolar lavage from a dog with a hypersensitivity reaction.
A, Note the abundant brightly staining eosinophils, in conjunction with less prominently staining cells. (Wright stain. Original magnification 200×.) B, Higher magnification of slide shown in A. Note the central neutrophil with pale eosinophilic staining cytoplasm and multilobulated nucleus. The eosinophils possess brightly staining eosinophilic granules, to the left an unlobulated nucleus, presumptive globule leukocyte, and to the right a trilobed nucleus, typical of eosinophils. (Wright stain. Original magnification, 1000×.)
Careful examination is required to distinguish eosinophils from neutrophils in some wash specimens. In thick areas where the cells are not well spread out, individual granules may be hard to see. If normal neutrophils are present, the contrast in cytoplasmic color is usually evident; however, caution must be exercised because the cytoplasm of neutrophils, especially in exudative samples, sometimes stains a diffuse, uneven, eosinophilic color. When differentiating these two cells, it is best to search for well-spread-out cells with definitive cytoplasmic granules instead of diffuse eosinophilic coloration. Individual granules are most readily observed in partially ruptured cells that are spreading out and are also free in the background of the smear (see Figure 16-9, B). In cats, eosinophils may be difficult to recognize because they tend to be tightly packed with slender, rod-shaped granules that are not as pronounced in color as those in dogs (see Figure 16-9, A). Eosinophils tend to be slightly larger than neutrophils, and their nuclei are less segmented (often bilobed or trilobed), which may aid in their identification (see Figures 16-9, A, and 16-10, B).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


