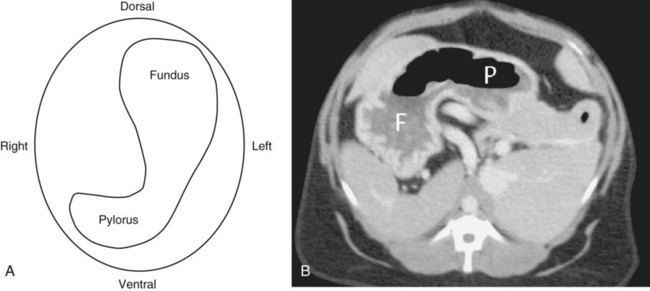
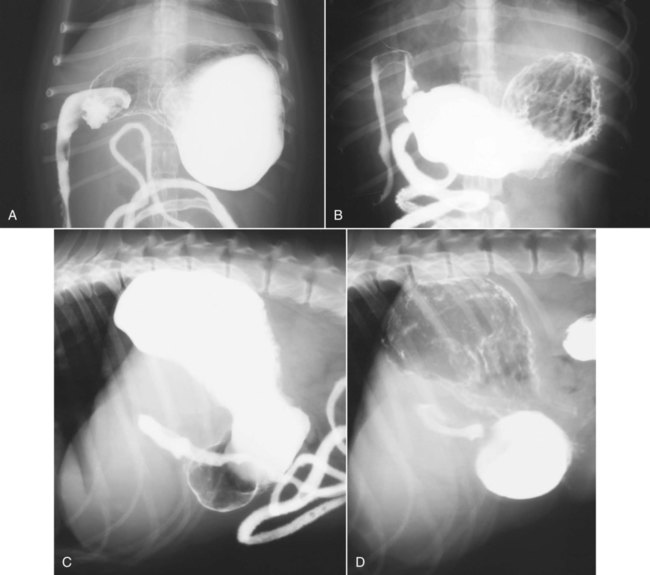
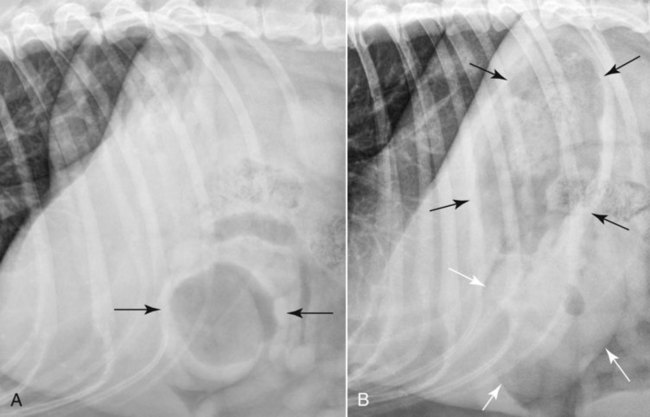
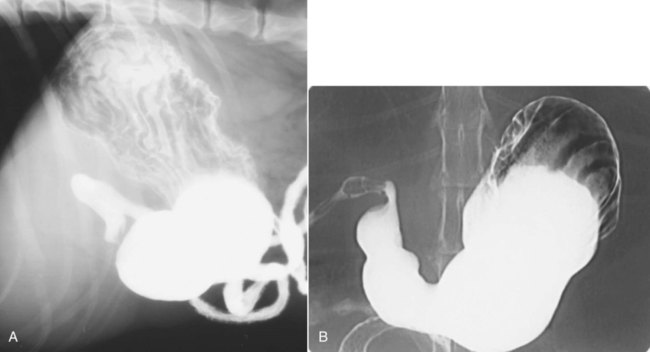
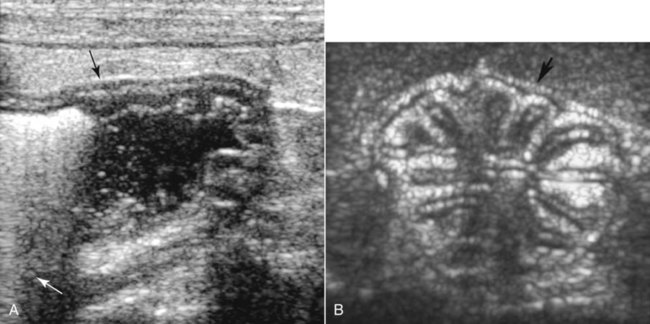
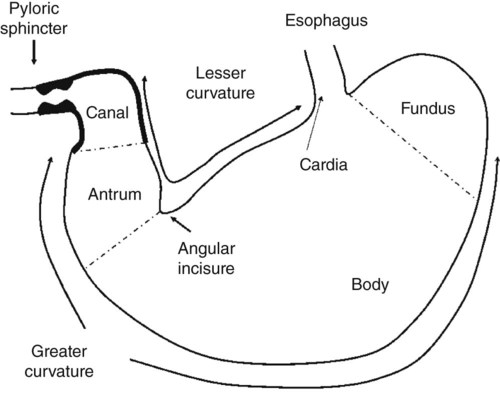
In the normal dog and cat, the empty stomach usually lies cranial to the last pair of ribs,1,2 but it may extend slightly caudal to the costal arch. The stomach lies in a transverse plane immediately caudal to the liver, primarily to the left of the median plane. The stomach is subdivided into the cardia, fundus, body, and pylorus (Fig. 43-1).1 The cardia is a small area at the esophagogastric junction. The fundus is the dome or outpouching from the left dorsal aspect of the stomach. The body is the middle portion from the fundus to the pyloric portion and is the largest portion of the stomach. The distal third of the stomach is the pyloric portion, which is further subdivided into the pyloric antrum and the pyloric canal. The pyloric antrum is the proximal two thirds of the pyloric portion and is relatively thin walled and slightly expanded. The pyloric canal, the distal third of the pyloric portion, is more muscular and contains a double sphincter. Additional landmarks of the stomach include the greater and lesser curvatures and the angular incisure (notch).1 The greater curvature is the convex surface of the stomach that originates at the cardia and extends caudoventrally around to the pylorus. The lesser curvature is the concave surface that originates to the right of the cardia and extends cranioventrally to the pylorus. It is the shortest distance between the cardia and the pylorus. The angular notch is the point of acute angulation of the lesser curvature, located approximately at the junction of the body and the pyloric antrum. The mucosal surface of the stomach is characterized by numerous folds or ridges called rugal folds or rugae. Ingesta within the stomach may obscure some lesions or simulate other lesions and thus create false-negative or false-positive results. Ideally, radiographic examination of the stomach should be performed on an animal that has fasted for 12 to 24 hours,3–5 but this is usually not practical, and in some patients fasting is contraindicated. A cleansing enema may be useful if a subsequent contrast study is contemplated. Fasting and enemas should be avoided in patients with acute abdominal disorders for which time delays are medically contraindicated or when fluid and gas patterns in the bowel may be of diagnostic importance. Also, many drugs used for treatment of gastrointestinal disorders or for sedation to facilitate radiographic positioning reduce gastric motility and may cause gas distention of the stomach. These preparations should be avoided or discontinued for an appropriate interval before any contrast study is undertaken.6–10 Survey radiographs may be sufficient for diagnosing some gastric abnormalities. If contrast studies are necessary, survey radiography should always precede them. Various special procedures to assess the stomach are available and include conventional barium sulfate gastrography, low-volume gastrography, double-contrast gastrography, pneumogastrography, gastrography with iodinated contrast media, and gastric-emptying studies with barium/food or radiopaque marker/food mixtures.2,3,6,11–23 See Box 43-1 for one method of performing a positive-contrast gastrogram. The stomach is easy to recognize by its location and shape and the content of gas, ingesta, or both. The entire stomach may not be discernible on survey radiographs if it is empty or if the gastric fluid content silhouettes with the liver or other abdominal structures. As a general guide, on the lateral view the axis of the stomach from the fundus through the body and pylorus is either perpendicular to the spine, parallel to the ribs, or somewhere between these angles (Fig. 43-2, A). On the lateral view, the pylorus may be superimposed over the body or located slightly cranial to the body. On the ventrodorsal view of the dog, the cardia, fundus, and body of the stomach are located to the left of midline, and the pyloric portions are located to the right of midline. The pyloric sphincter usually is located in the right cranial abdominal quadrant at approximately the level of the tenth or eleventh ribs and is usually cranial to the pyloric canal.2 In immature dogs the pylorus may be located closer to midline than in adults.11 In ventrodorsal radiographs, the long axis of the stomach is generally perpendicular to the spine with the stomach running transversely across the abdomen, making the angular notch difficult to identify (Fig. 43-2, B). The stomach may also have a U-shaped appearance with a more obvious angular notch and still be within its normal location. On the ventrodorsal view of the cat, the stomach is more acutely angled with the pylorus located at or near the midline (Fig. 43-2, C). Variations in the appearance of the stomach in the dog based on the shape of the thorax and cranial abdomen (i.e., breed conformation) have been described.2 The shape of the stomach also varies with the degree of gastric distention. One of the most important factors in the appearance of the stomach is the position of the patient during radiography.24 This is an important concept that must be understood for accurate interpretation of radiographs and for demonstration of some gastric lesions. Variation in appearance of the stomach with different patient positions is caused by shifts in fluid and gas distribution within the stomach. The stomach usually contains both fluid and gas, with the fluid being either of soft tissue or mineral opacity. This fluid and gas distribution varies with the position of the patient because fluid settles dependently because of gravity, and gas rises to the highest part of the lumen. Gas and positive-contrast medium are relatively easy to visualize on radiographs, whereas fluid within the stomach may be more difficult to see because it may cause border effacement with other structures of similar opacity. To optimize the amount of information provided by fluid and gas shifts, obtaining right and left lateral radiographic projections routinely, along with a ventrodorsal radiograph, is recommended.25 This was discussed in Chapter 35. To understand the radiographic appearance of the stomach, it should be visualized as lying in a transverse plane with the fundus located dorsally and on the left and the pylorus ventrally and on the right (Fig. 43-3). Thus, for example, with a patient in dorsal recumbency for a ventrodorsal view, fluid within the lumen settles dependently to the fundus and body of the stomach. Gas rises to the uppermost portion, which with the patient in dorsal recumbency is in the pyloric antrum and the body near midline. Figure 43-3, B is a transverse computed tomographic image of the cranial abdomen at the level of the stomach acquired with the dog in dorsal recumbency. Note the fluid opacity filling most of the stomach with the gas bubble floating near midline. With this image as a starting point, it is possible to predict how the fluid and gas would be distributed if the animal were rotated in 90-degree increments for a left recumbent lateral view, a dorsoventral view in sternal recumbency, a right recumbent lateral view, and back to a ventrodorsal view in dorsal recumbency. These variations in appearance of the stomach are altered further by the volume and ratio of fluid to gas within the stomach. Examples of the appearance of the stomach with various views are illustrated in Figures 43-4 and 43-5; these views were made with a vertically directed x-ray beam. In Figure 43-4, barium is present to facilitate understanding how the fluid shifts as a function of gravity. On the ventrodorsal view (Fig. 43-4, A), gas is located in the pylorus and the body near midline. Fluid gravitates to the fundus; some fluid may be trapped in the pyloric antrum in a ventrodorsal view, but this is usually minimal. On a dorsoventral view (Fig. 43-4, B), gas rises to the fundus, and fluid settles dependently to fill the pyloric portions and part of the body. On the left recumbent lateral view (Figs. 43-4, C, and 43-5, A), gas rises to the pyloric portion of the stomach, and fluid settles dependently to the fundus and body. A gas pocket may be trapped occasionally in the fundus in a left lateral view. The fundus and/or body may be difficult to see in a left lateral view because of the intraluminal fluid silhouetting with adjacent structures. (see Fig. 43-5, A). On the right lateral view (Figs. 43-4, D, and 43-5, B), gas rises to the fundus and body, and fluid settles dependently to fill the pyloric portions and part of the body of the stomach. In a right lateral view, the pyloric portion is well visualized with positive-contrast medium. The pyloric antrum and distal part of the body may appear occasionally as a soft tissue mass in the right lateral view (see Fig. 43-5, B). If a mass or foreign body is suspected on a right lateral view in the pylorus, a left lateral view should be made to better visualize this area as gas will fill the pylorus. Recognizing that variations from factors, such as the position of the patient and the volume and ratio of fluid to gas within the stomach, exist in the appearance of the normal stomach is important. The ability to take advantage of fluid and gas shifts within the stomach to visualize certain portions of the stomach more clearly is also important. Table 43-1 is a simplified summary of the expected changes in gas and fluid within the stomach on change in patient position. Table • 43-1 Rugal folds are seen inconsistently on survey radiographs. With positive-contrast gastrography, rugal folds are best seen at the peripheral portions of the stomach, where they may be visualized end-on as regular small filling defects at the mucosal surface. If projected en face, rugal folds are not visible with positive-contrast gastrography unless the barium is well penetrated by the x-ray beam, or there is only a small amount of barium in the stomach. Rugal folds then appear as relatively radiolucent, linear filling defects separated by barium in the interrugal spaces (Fig. 43-6). Radiographic assessment of rugal folds is subjective because they vary in size and number,5,26 and their appearance depends on the degree of gastric distention. Rugal folds are more tortuous in the nondistended stomach and become more uniform and parallel to the gastric curvature with increasing distention.5,12 Rugal folds are smaller and more spiral in the pyloric antrum.27 Rugal folds may not be visible if the stomach is overdistended.13 Rugal folds are smaller and fewer in number in cats than in dogs.2 A reference range for normal rugal-fold thickness in dogs weighing 2 to 50 kg has been reported to be 1 to 8 mm.26 After administration of barium, gastric emptying should start within 15 minutes in most normal patients.2,28,28 During gastrography with barium sulfate, the stomach generally empties within 1 to 4 hours in dogs.6,28 Rapid emptying of the stomach has no clinical significance, whereas delayed emptying is potentially of much greater significance. The rate of gastric emptying is a complex phenomenon that is altered by the volume of contents, chemical and physical properties of chyme entering the duodenum, various reflex mechanisms, certain medications, and the type of contrast medium used. Thus a standard approach must be used to evaluate the rate of gastric emptying radiographically. Because the stomach starts to empty faster with an increased intraluminal volume,14 the dosage of contrast medium for a barium study must be standardized. Low dosages may result in delayed gastric emptying, which leads to a false impression of pyloric obstruction. If a standard technique has been used, and no medications that affect gastric emptying were administered, then delays in gastric emptying are likely related to psychological influences or disease at the pylorus. Emotional stress and noise may inhibit gastric movement.30 Anxiety, fear, rage, or pain induced by physical manipulation of the patient, gastric intubation, and physical restraint may contribute to temporary delayed gastric emptying. Thus patients with delayed gastric emptying must be allowed to calm down in a quiet environment before diagnostic significance is placed on this finding. For these reasons, minimal significance is usually placed on slight or minor delays in gastric emptying if the stomach proceeds to empty in a normal manner after an initial delay. Studies that use barium-food mixtures have been performed to evaluate gastric function further.15,16 Emptying times for individual dogs were repeatable; however, the range of normal gastric emptying was so wide (7 to 15 hours) that this procedure is not useful for evaluation of gastric emptying unless gross abnormalities are present.15 Gastric emptying times for dogs and cats can vary from 4 hours for high-moisture food to 16 hours for dry food.5 An alternative technique for evaluating gastric emptying of solids in dogs and cats has been developed by using radiopaque barium-impregnated polyethylene spheres (BIPS, Chemstock Animal Health Ltd., Christchurch, New Zealand) mixed with food.20–23 The number and size of radiopaque spheres, type and amount of food, and fasting period must be standardized. An advantage of the BIPS technique is that it can be performed in most veterinary practices; however, study times may be long (up to 10 hours). Some controversy exists about the usefulness of BIPS for gastric emptying analysis, and these studies should be interpreted by a specialist. Scintigraphic evaluation of gastric emptying of food may be considered the gold standard technique. Scintigraphy can be completed in 4 to 5 hours, but availability is limited.9,31,31 Gastric emptying time is significantly different in cats versus dogs as measured by BIPS compared with scintigraphy. Emptying times measured by BIPS were significantly longer relative to scintigraphy.33,34 A radiolucent line occasionally can be seen within the stomach wall of the cat because of submucosal fat.35 Ultrasound is a useful addition to radiography for evaluation of the gastrointestinal tract. It may eliminate the need for barium studies because gastric motility; wall thickness and architecture; and, to a lesser extent, luminal contents may be evaluated sonographically. In addition, ultrasound examination is quicker than an upper gastrointestinal series and may be equally sensitive and specific for detection of gastric disease.36 Gas and ingesta within the stomach may obscure the far wall, but the lumen and far wall can be evaluated in those patients in which the stomach contains fluid and little gas (Fig. 43-7, A). Ideally, sonography should be performed after a 12-hour fast and before barium is administered. If needed, intraluminal gas can be removed by an orogastric tube and the stomach distended with fluid to act as an acoustic window.37,38 The stomach should be scanned in longitudinal and transverse planes. For evaluating stomach wall layers, 7.5 MHz (or higher) transducers are preferred, but 5 MHz transducers may be needed to evaluate deeper portions of the stomach. Ultrasound has been used to help diagnose gastric neoplasms,39–46 inflammation or infection,47 ulcers,48 foreign bodies,45,49 pyloric hypertrophy,50 gastric mineralization,51 and gastroduodenal and gastrogastric intussusceptions,52,53 and to evaluate gastropexy sites.54,55 The appearance of the stomach varies with the amount of distention and the extent of luminal contents. When empty, the stomach may have a wagon-wheel appearance because of infolding of rugal folds (Fig. 43-7, B). This is especially noticeable in the cat, and the empty stomach is sometimes mistaken for an abnormal kidney by inexperienced sonographers. With increasing distention, rugal folds become less conspicuous. Stomach wall thickness in dogs is 3 to 5 mm depending on the location and size of the dog, with larger dogs having a thicker stomach wall.37,56 In cats, the rugal-fold thickness has been reported as 4.4 mm,57 2.6 mm,57 or 2.0 mm58 for the interrugal area and 2.1 mm for the pylorus.58 Five wall layers corresponding to the mucosal surface, mucosa, submucosa, muscularis propria, and subserosa/serosa can be identified.37 These layers have alternating hyperechoic and hypoechoic appearances, with mucosal surface, submucosa, and subserosa/serosa being hyperechoic and the mucosa and muscularis layers being hypoechoic (see Fig. 43-7). The mean number of peristaltic contractions observed ultrasonographically in dogs has been reported to be 4 to 5 contractions per minute.37 Because the stomach is in close apposition with the liver, changes in size or position of the liver may cause a change in position of the stomach. Generalized hepatomegaly often produces caudal and dorsal displacement of the stomach.59 This displacement may be asymmetric if caused by a mass.2 However, because the cardia is relatively fixed, even generalized hepatomegaly produces a nonuniform displacement of the stomach. Thus on the lateral view, generalized hepatomegaly often produces caudal and dorsal displacement of the pylorus and body of the stomach. This displacement changes the axis of the stomach so that the axis is no longer parallel with the ribs (Fig. 43-8, A). On the ventrodorsal or dorsoventral view, generalized hepatomegaly often causes displacement of the body and pylorus of the stomach caudally and toward the left (Fig. 43-8, B
The Stomach
Anatomy
Radiographic Examination
Preparation
Radiographic Technique
Normal Radiographic Findings
RADIOGRAPHIC VIEW
LOCATION OF GAS
LOCATION OF FLUID
Dorsoventral
Fundus
Body/pylorus
Ventrodorsal
Body (± pylorus)
Fundus
Left recumbent lateral
Pylorus (± body)
Fundus
Right recumbent lateral
Fundus
Pylorus
Ultrasonographic Examination
Normal Ultrasonographic Findings
Abnormal Radiographic and Ultrasonographic Findings
Displacement
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Veterian Key
Fastest Veterinary Medicine Insight Engine