Chapter 1. The principles and practice of ocular pathology
OBJECTIVES
• To characterize the case material seen in an ocular pathology service
• To present the basics of tissue handling
• To present the nuts and bolts of an ocular pathology service.
GENERAL POINTS
Throughout this book, when relevant, the collection of the Comparative Ocular Pathology Laboratory of Wisconsin (COPLOW) will be referenced to provide data regarding the relative numbers for categories of disease. The COPLOW collection as it exists at January 2008 will be used. Throughout the book, at the conclusion of each chapter, readers seeking further detail will find lists of suggested published texts, papers and other source material. It should be noted that these lists are intended to be illustrative, rather than exhaustive.
Comparative Comments
Comparative Comments
Most human ocular pathology laboratories handle all of the tissue removed by ophthalmologists. In addition to globes, there are exenteration specimens, including the lids and orbital contents, or the contents of the globe after evisceration surgery. The majority of specimens, however, are skin lesions, conjunctival lesions, and orbital lesions following incisional or excisional biopsy.
Characteristics of eyes submitted to the COPLOW pathology service
Reasons for submissions: Most submissions are from animals where the globes have been enucleated in the interest of the patient with the following justifications:
• Blind, non-cosmetic and painful eyes
• To facilitate the diagnosis of a systemic disease, e.g. blastomycosis
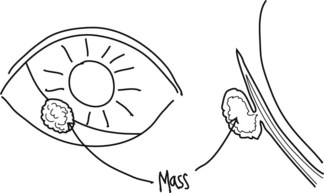
• To remove a mass lesion perceived to represent a threat to the general health of the animal, should local invasion or metastatic disease subsequently occur.
Species represented include:
• 68% canine (15 016 cases)
• 24% feline (5203 cases)
• 4% equine (758 cases)
• 4% other (1.2% avian).
Tissue:
• Enucleated globes: 67%
• Evisceration specimens: 10%
• Other specimens: 23%
Disease type (these categories are not mutually exclusive):
• Neoplasia: 39%
• Glaucoma: 34%
• Inflammation: 29%
• Trauma: 15%
• Congenital disease: 2%.
Characteristics of conditions infrequently encountered in the pathology laboratory
Conditions that have largely cosmetic implications:
• Breed-related pigmentary variations
• Congenital abnormalities where vision and comfort are not impacted and which remain static
• Non-progressive focal lesions, e.g. corneal scars.
Conditions that may be successfully treated by means other than enucleation or excision including:
• Inflammatory conditions amenable to medical therapy, e.g. chronic superficial keratitis (Fig. 1.1)
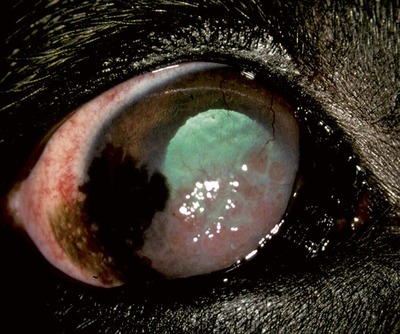 |
| Figure 1.1 Canine chronic superficial keratitis (degenerative pannus). This potentially blinding disease is seen frequently, but treated successfully with anti-inflammatory topical medications and seldom results in a pathology submission. German Shepherd dog, 5 years old: the right cornea illustrates temporal pigment with a cellular infiltrate and neovascularization extending nasally. |
• Cataract: cataracts are generally removed surgically by phaco-emulsification and specimens are seldom submitted for histopathology
Conditions that may affect vision but rarely necessitate eye removal, such as:
Comparative Comments
• Retinal degenerations, including progressive retinal atrophy (Fig. 1.2)
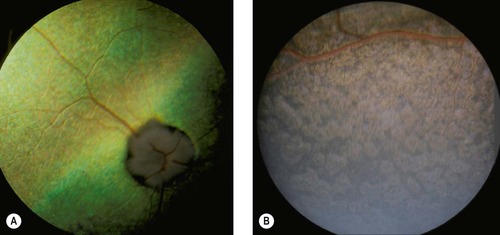 |
| Figure 1.2 Progressive retinal atrophy (PRA). Funduscopic images of two cases of canine progressive retinal atrophy. There is no advantage to removing the eye from an affected dog. The pathologist is occasionally asked to verify that there is retinal atrophy when the eye is removed for other reasons or in globes removed at necropsy. By this time, the atrophy might be end-stage, when the best diagnosis is that the atrophy may or may not be compatible with PRA. (A) Akita, 2.5 years old: photographed with a neutral density filter, the tapetum is hyperreflective, retinal vessels are attenuated, and the optic disc is pale. (B) Labrador Retriever, 3 years old: the non-tapetal retina has a cobblestone appearance caused by depigmentation and pigment clumping of the retinal pigment epithelium (RPE). |
• Chronic but inactive keratitis
• Optic neuritis or compression without progressive disease.
Comparative Comments
A large percentage of the globes removed and submitted to a human ocular pathology laboratory is composed of blind eyes following surgical or non-surgical trauma. Others represent end-stage diabetes, glaucoma, vascular occlusion, retinopathy of prematurity, phakomatoses, and malignant tumors. Criteria for enucleation are similar in that, except in the case of neoplasia, only blind eyes that are painful and/or disfiguring are generally removed.
COPLOW RECOMMENDED TISSUE HANDLING PROCEDURES (Figs 1.3, 1.4)
 |
| Figure 1.4 Keratectomy specimens mounted flat on plastic. These specimens from the left and right eyes are mounted on a non-absorbent surface, which will allow them to fix flat and rigid and make orientation easier. |
Enucleated globes
• Immediately dissect all extraneous tissues from the globe, unless directly involved in the pathologic process or considered important for orientation, e.g. conjunctival squamous cell carcinoma or an orbital meningioma
• Identify the location of the lesion of interest with a suture or a mark or provide a simple drawing.