Chapter 37The Metacarpal Region
Anatomy
This chapter discusses the examination and diagnosis of injuries to the metacarpal region of the horse. The detailed anatomy of the deep digital flexor tendon (DDFT) (see Chapter 70), the accessory ligament of the deep digital flexor tendon (ALDDFT) (see Chapter 71), the superficial digital flexor tendon (SDFT) (see Chapter 69), and the third interosseous muscle or suspensory ligament (SL) (see Chapter 72) is discussed elsewhere.
The proximal aspect of the third interosseous muscle or SL attaches to the proximal palmar aspect of the McIII and the palmar carpal ligament and lies between the McII and McIV. Large exostoses on the axial aspect of the McII or the McIV have the potential to impinge on the abaxial border of the SL. The carpal sheath (see Chapter 75) extends through the proximal third of the metacarpal region. The amount of fluid in the carpal sheath varies between horses but is usually bilaterally symmetrical.
Diagnosis
Local Analgesic Techniques
Intrathecal analgesia of the DFTS usually results in improvement in lameness associated with pain from within the sheath, but a better response is frequently seen after perineural analgesia of the palmar and palmar metacarpal nerves. Injection into the DFTS is most easily performed on the palmar midline of the pastern region, distal to the proximal digital annular ligament. The likelihood of inducing iatrogenic hemorrhage at this site is small, and retrieval of synovial fluid usually is easier than from the DFTS proximal to the PAL. If distention of the DFTS is only mild, compression of the proximal part of the sheath by an assistant to increase distention in the palmar pouch in the pastern can be helpful. Injection into the carpal sheath is usually only indicated if the sheath is distended (see Chapter 75).
Imaging
Radiography and Radiology
Superimposition of the McII and McIV over the McIII can create confusing radiolucent Mach lines (see page 174). The nutrient canal in the McII and McIV varies in prominence6 and should not be confused as a fracture. Ossification varies between the McII and McIV and the McIII in normal horses.
Ultrasonography
Ultrasonographic examination of the metacarpal region is discussed in detail elsewhere (see Chapters 16 and 69 to 72). In large, cob-type horses, the skin and underlying subcutaneous tissues in the metacarpal region may be thick, making it difficult to obtain high-resolution images. Dense stubble may persist after fine clipping of the hair coat, making it difficult to maintain good contact. Deep skin folds may further complicate the issue. For these horses it may be necessary to amplify the power and gain controls of the ultrasound machine and increase the focal depth of the transducer. Image quality may be enhanced by application of copious amounts of the ultrasound coupling gel to the skin for at least 15 minutes before imaging.
Differential Diagnosis
Bucked or Sore Shins and Saucer (Dorsal Cortical) Fractures of the Third Metacarpal Bone
See Chapter 102 for a discussion of bucked shins and dorsal cortical (saucer) fractures of the McIII.
Medial and Lateral Condylar Fractures of the Third Metacarpal Bone
See Chapter 36 for a discussion of medial and lateral condylar fractures of the McIII (see page 408).
Incomplete, Longitudinal Palmar Cortical Fatigue Fractures of the Third Metacarpal Bone and Stress Reactions
Diagnosis
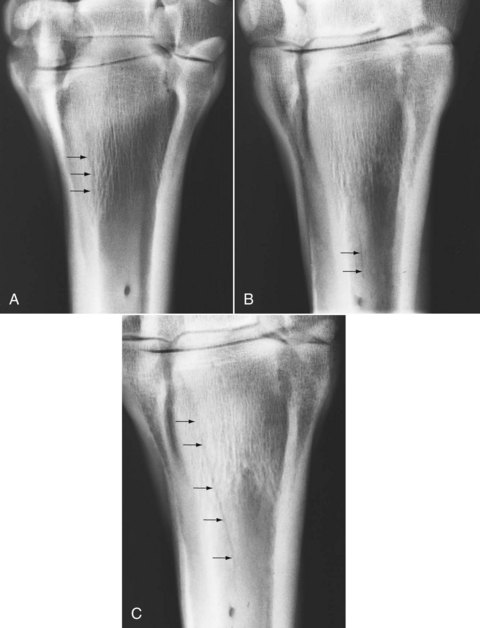
Dorsopalmar radiographic images of the proximal metacarpal region may reveal increased radiopacity of the proximal medial aspect of the McIII, with or without a longitudinal radiolucent line extending a variable distance proximodistally (Figure 37-1). If present, the radiolucent line is invariably located medial to the axis of the McIII. Several slightly oblique dorsopalmar images may facilitate identification of a fracture. Generally no radiological abnormality is detectable in other images, although very occasionally periosteal callus is seen on the palmar aspect of the McIII in a lateromedial image. In some horses, no detectable radiological abnormality exists at any stage.
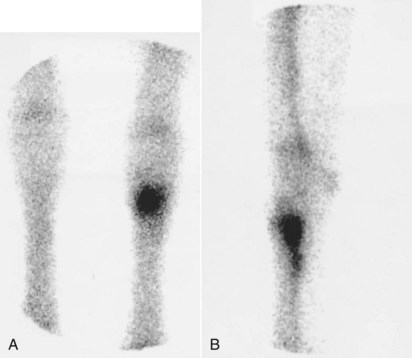
Diagnostic ultrasonography usually reveals no detectable abnormality. Rarely a defect in the palmar cortex of the McIII can be identified. Nuclear scintigraphic images usually demonstrate moderate to intense IRU in the proximal palmar aspect of the McIII in dorsal and lateral bone phase images (Figure 37-2). Early radiopharmaceutical uptake in the proximal palmar aspect of the McIII may also be evident in pool phase images. This pattern of uptake is indistinguishable from that associated with an avulsion fracture of the McIII at the attachment of the SL. It is not known whether horses without radiological change, but with scintigraphic evidence of an increased bone modeling in the proximal aspect of the McIII, would develop a radiologically evident incomplete palmar cortical fracture of the McIII if the horses were kept in work, or whether this is a different manifestation of the response of bone to exercise.
Midshaft Fractures of the Third Metacarpal Bone
See page 502 for a discussion of midshaft fractures of the McIII.



