Chapter 75The Carpal Canal and Carpal Synovial Sheath
Anatomy
Fluid within the sheath may be seen readily by ultrasonography between the DDFT and its accessory ligament in normal horses, with no palpable distention of the sheath wall.2 Within the proximal part of the carpal sheath, the SDFT and DDFT contain muscular tissue and therefore have hypoechoic regions within them on ultrasonographic examination.3-5 However, the ALSDFT is uniform in its echogenicity.4,5 The position of the accessory carpal bone prohibits ultrasonographic examination from the caudal aspect of the carpus. The carpal sheath and its contents are evaluated most easily from the distal caudomedial aspect of the antebrachium and carpus and the palmar aspect of the proximal metacarpal region. The heterogeneous echogenicity of the digital flexor tendons proximally can make definitive diagnosis of a tendon lesion difficult, but comparison with the contralateral limb may be helpful. Endoscopic evaluation may yield further information and permit surgical debridement of torn fibers (see Chapter 24).
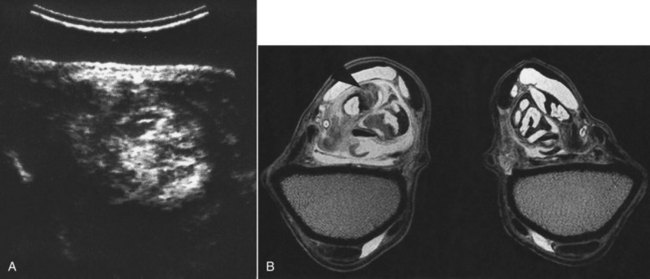
Occasionally abnormalities cannot be detected using conventional imaging techniques and magnetic resonance imaging (MRI) is required (see Figure 75-1, B). Normal MRI anatomy of the carpal region has recently been described.6