Chapter 109The European and Australasian Standardbreds
 The European Standardbred
The European Standardbred
Dimensions and Characteristics
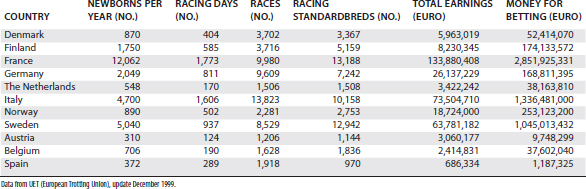
The European Standardbred (STB) is historically the result of different crosses between the classic American bloodlines and European families. The French STB is known for its stamina and aptitude for long distances. The American-derived families, however, have been selected for speed and racing at a fixed distance of 1 mile and are represented more widely in Italy and Sweden. Several countries (especially France, Italy, Germany, and the Scandinavian countries) have developed individual bloodlines and today are able to produce good-quality STB trotters. In Europe no races are available for pacers. In Table 109-1 the STB population and racing activity of different European countries are listed.
TABLE 109-1 Distribution of Standardbreds Born in Different European Countries, Summary of the Racing Activity, Earnings, and Betting
 -mile) tracks, and no 1-mile racetracks (with the exception of training centers) are present in Europe. The most characteristic and popular racetrack is the Plateau de Gravelle in Vincennes, Paris, where the Prix d’Amerique is held. The track surface is made of pressed charcoal powder; slopes and descents are present; and the circuit is egg-shaped, which is unique in Europe, where other racetracks have a regular design. Another famous French racetrack, Cagnes-sur-Mer in Nice, is well known for being 1200 m in length and for hosting the Criterium de Vitesse, one of the main European free-for-all races. In Sweden, Solvalla racetrack in Stockholm represents the heart of the Swedish STB racing, and in late May the multiple-heat race Elitlopp is held. In Norway, in addition to well-developed STB racing (the main racetrack being Bjerke near Oslo), races for Warmblood horses (a breed historically devoted to hard work but now genetically selected for speed) are still popular and meet the special interest of the local public.
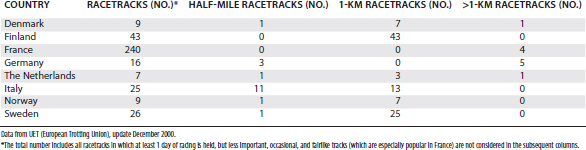
-mile) tracks, and no 1-mile racetracks (with the exception of training centers) are present in Europe. The most characteristic and popular racetrack is the Plateau de Gravelle in Vincennes, Paris, where the Prix d’Amerique is held. The track surface is made of pressed charcoal powder; slopes and descents are present; and the circuit is egg-shaped, which is unique in Europe, where other racetracks have a regular design. Another famous French racetrack, Cagnes-sur-Mer in Nice, is well known for being 1200 m in length and for hosting the Criterium de Vitesse, one of the main European free-for-all races. In Sweden, Solvalla racetrack in Stockholm represents the heart of the Swedish STB racing, and in late May the multiple-heat race Elitlopp is held. In Norway, in addition to well-developed STB racing (the main racetrack being Bjerke near Oslo), races for Warmblood horses (a breed historically devoted to hard work but now genetically selected for speed) are still popular and meet the special interest of the local public.A variety of track designs and purposes are present in Europe. For example, a large number of small country tracks are found in France, and local races are organized in a fairlike fashion, whereas the main racing activity is concentrated in Paris. In Italy, however, important races have a more even distribution among racetracks, Milan and Rome being the main places. In Table 109-2 the distribution of racing tracks in the main European countries is summarized.
Lameness Examination
A basic lameness history must include the following:
Concerning conformation, the clinician should check the following:
Diagnostic Imaging
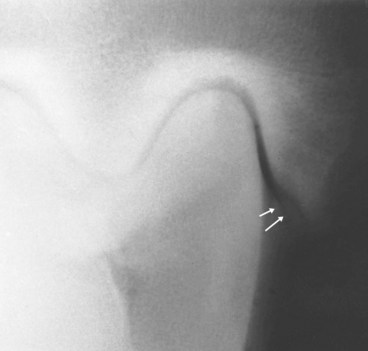
Common pathological findings in the distal limb of European trotters include osteophyte formation on the distal aspect of the middle phalanx, sometimes associated with modeling of the extensor process of the distal phalanx, as seen on a lateromedial image of the foot (Figure 109-1). This radiological pattern often is associated with heel growth proceeding faster than toe growth (club foot). When associated with a positive lower limb flexion test and lameness abolished using analgesia of the DIP joint, this radiological finding is important and indicates the presence of OA. Fragmentation of the extensor process of the distal phalanx has controversial clinical significance, but in my experience these fragments cause synovitis of the DIP joint and should be removed using arthroscopy.

The flexed lateromedial image of the metacarpophalangeal or metatarsophalangeal joints is useful in evaluating lesions of the distal aspect of the McIII or the MtIII. In the hindlimb, the oblique images must be acquired in a proximal to distal direction (down-angled) to see better the area between the proximal phalanx and the base of the PSBs. Fragmentation of the proximal plantar aspect of the proximal phalanx represents a major cause of subtle hindlimb lameness (Figure 109-2).

A dorsopalmar image of the carpus helps to evaluate the proximal suspensory origin from the McIII, and focal or diffuse increased radiopacity of the McIII may be found (Figure 109-3). In yearlings and young horses, this image allows examination of the distal radius, and pathological modifications of the growth plate on the medial side (physitis) are a frequent cause of early lameness. The most common lesions of the carpus are seen with the dorsolateral-palmaromedial oblique image and the dorsal 35° proximal-dorsal distal oblique (skyline) image of the flexed carpus to highlight the distal row of carpal bones. The radiographs must be of excellent quality, and the appropriate projection must be obtained because false-negative radiographic images are frequent. Abnormal findings include areas of radiolucency in the dorsoproximal articular border of the radial fossa of the third carpal bone, radiolucent lines suggestive of fractures, and increased radiopacity of the third carpal bone.5 A moderate degree of increased radiopacity in the radial fossa of the third carpal bone is considered normal in racing horses, but more severe increased radiopacity associated with radiolucent areas represents a pathological finding.6,7

In the hindlimb the centrodistal and tarsometatarsal joints frequently appear normal radiologically even when distal hock joint pain is diagnosed clinically as the source of pain. Scintigraphy is an excellent tool for diagnosing OA of these joints.8 The tarsocrural joint is a predilection site for OC in STBs, and the presence of fragments associated with effusion may represent an indication for arthroscopic surgery. Lesions affecting the lateral trochlear ridge of the talus and medial malleolus of the tibia more frequently cause lameness and effusion than do those of the cranial aspect of the intermediate ridge of the tibia. In horses with effusion but without obvious fragmentation, a specific dorsal 10° to 15° lateral-plantaromedial oblique image is required to evaluate the axial aspect of the medial malleolus. Subtle osteochondral fragmentation or radiolucency easily can be overlooked (Figure 109-4).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


