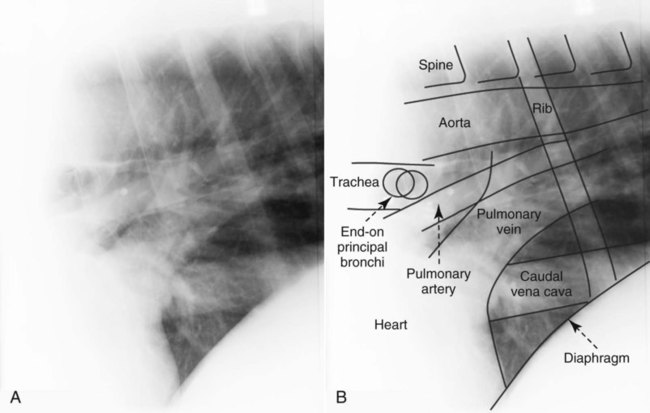
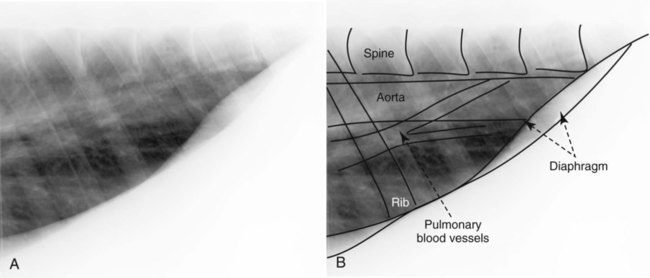
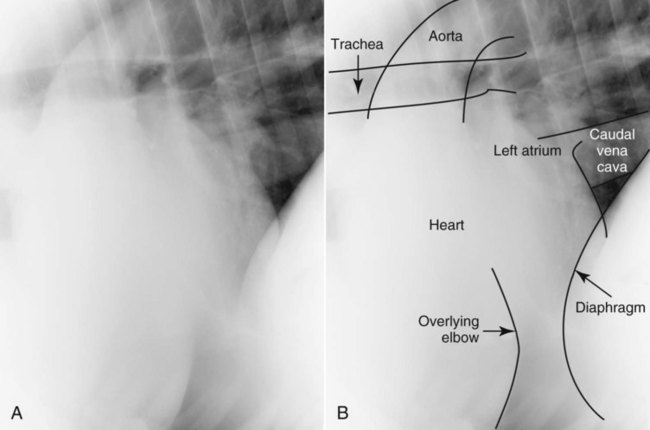
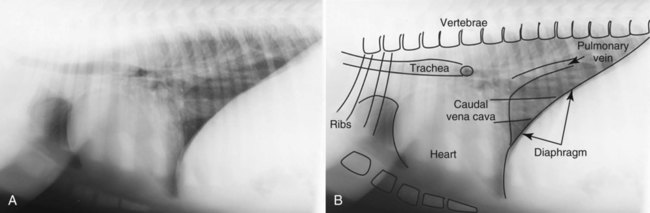
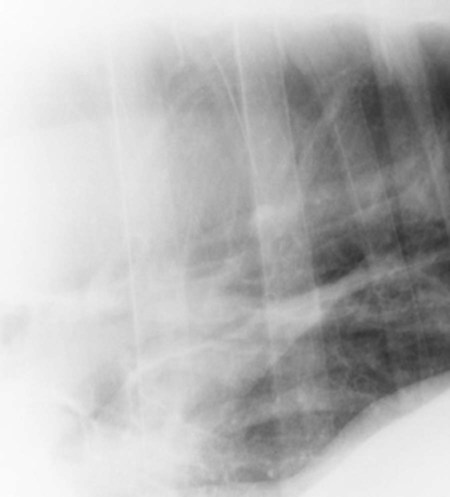
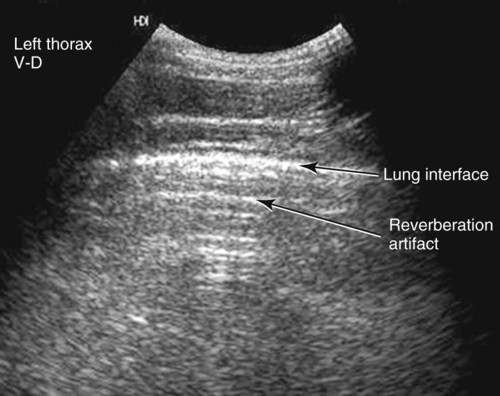
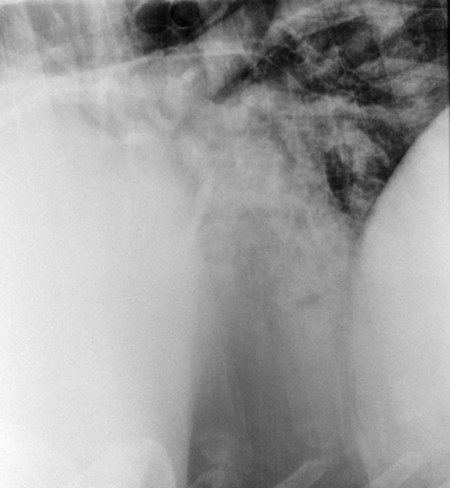
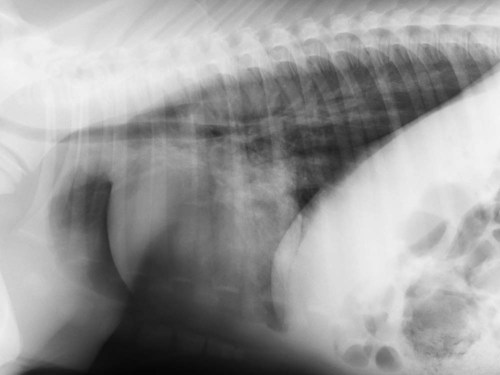
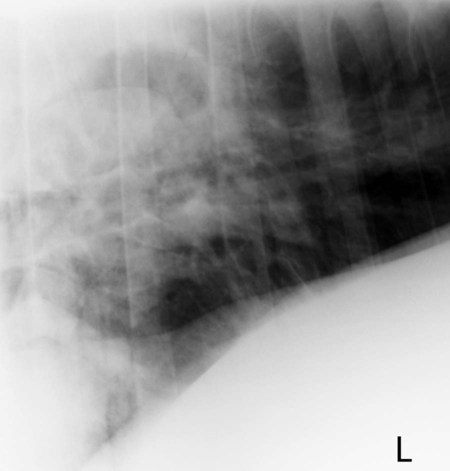
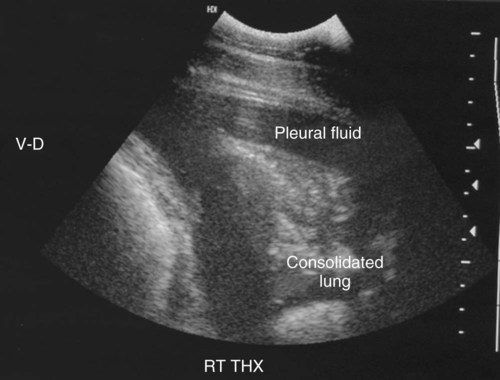
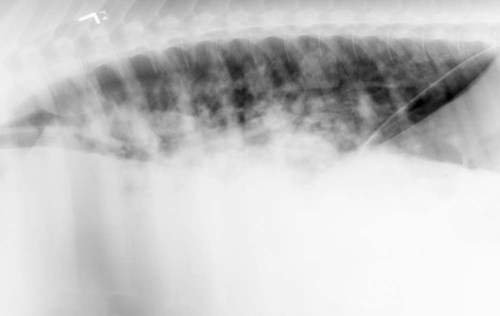
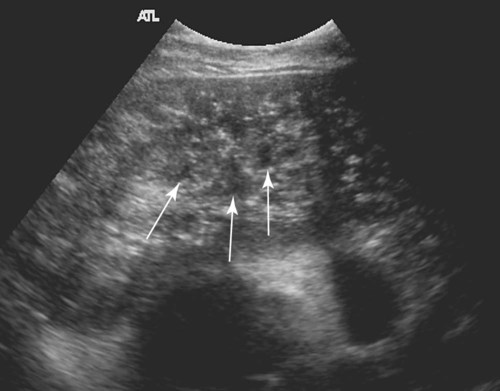
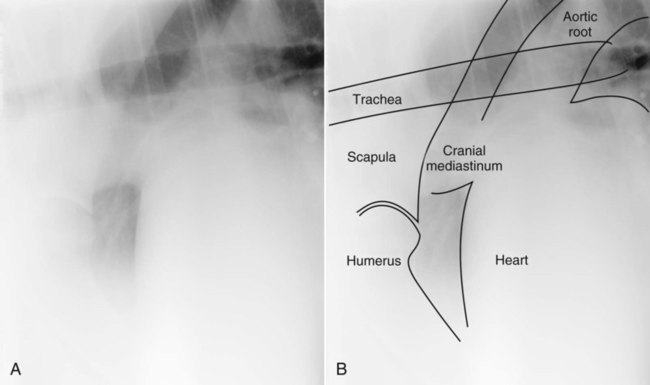
Technical aspects of radiographing the equine thorax are covered in Chapter 25, but important principles are reiterated here. Radiographing the entire thorax of an adult horse requires a grid and large stationary x-ray tubes that are generally available only at referral centers. Portable radiographic tubes require an excessively long exposure time to penetrate the adult thorax; this usually results in motion artifact, rendering the images nondiagnostic. Four overlapping 14-inch × 17-inch views are usually required to image the entire thorax of an adult horse. They are acquired in the craniodorsal, caudodorsal, caudoventral, and cranioventral aspects of the thorax (Fig. 34-1). In addition to these standard views, radiographs centered over any identified lesions may also be useful. When thoracic radiographs are obtained in a standing horse, the lung closest to the cassette is seen most clearly. This occurs because the large width of the equine thorax results in the lung farthest from the cassette being magnified and blurred to the extent that even large lesions can be obscured. This is opposite to the situation in lateral radiographs of dogs and cats where lesions in the nondependent lung (i.e., farthest from the cassette) are seen most clearly because of the atelectasis that occurs in the dependent lung. This was also discussed in Chapter 25. In the horse, therefore, left-right and right-left radiographs are necessary to assess both the left and right lungs adequately.1 Radiographic exposure and degree of inspiration play an important role in the interpretation of thoracic radiographs and must be considered both for initial and serial radiographic examinations. As the quality of the radiograph improves, the amount of perceived interstitial lung pattern decreases.2 If a radiograph is underexposed or obtained during expiration, the lungs will appear diffusely more opaque than normal, mimicking a mild diffuse interstitial lung pattern often mistaken for disease. If the radiographs are overexposed, small or mild lung lesions may be obscured. The dorsal portion of the heart, descending aorta, caudal vena cava, hilar pulmonary arteries and veins, trachea, and carina are visible (Fig. 34-2). The hilar portions of the lungs are visible but are difficult to evaluate because of the superimposition of the heart and blood vessels. This view provides the largest unobstructed view of the lungs (Fig. 34-3). The normal equine lung has a mild diffuse bronchointerstitial lung pattern when compared with canine and feline lungs. The pulmonary blood vessels should be seen clearly, tapering toward the periphery of the lung field. The caudal borders of the heart, left atrium, caudal vena cava, pulmonary veins, and pulmonary arteries are evident on this view (Fig. 34-4). A small triangle of lung bounded by the caudal vena cava, caudal border of the heart, and cranioventral aspect of the diaphragm is evident. Because of the cardiac notch, no pulmonary markings are present over the central portion of the heart. The absence of pulmonary blood vessels in this region should not be mistaken for lung consolidation. The diaphragmatic reflection of the pleura follows the costochondral junctions to approximately the ninth rib and then travels dorsally, paralleling the costal arch to the middle of the last rib.3 This means that the normal lung does not extend ventral to the costochondral junction and, in fact, usually ends approximately 4 inches above the costochondral junction in adult horses at rest. Ventral to the costochondral junction is mediastinal fat that provides contrast between the caudal border of the heart and the diaphragm. This fat opacity should not be mistaken for pleural or pulmonary disease. The cranial portions of the lung, cranial mediastinum, aortic arch, and trachea are evident on this projection (Fig. 34-5). The lung is difficult to evaluate in this region because of the superimposition of the thoracic limbs. With the exception of evaluating for a mediastinal mass, this is typically the least helpful of all projections. When radiographed immediately after parturition, foals have a mild diffuse interstitial lung pattern because of incomplete expansion of the lungs, fluid in the small airways, and the uptake of fetal alveolar fluid in the interstitium (Fig. 34-6). This opacity should resolve within 6 hours of birth.4–6 The thymus is large in foals and can sometimes be seen as a soft tissue opacity cranial to the heart. The thymus is largest at approximately 2 months of age and should regress as the foal ages.5 Atelectasis occurs rapidly when foals are placed in lateral recumbency. This will result in the lungs of recumbent foals appearing more opaque than those of standing foals.5 Age, size, and phase of respiration all affect the radiographic appearance of the lungs. Many adult horses with normal respiratory function and no clinical signs of respiratory disease have a mild, diffuse bronchointerstitial lung pattern as a normal variation.2,7 This opacity may be caused by the slightly more abundant lobulation and connective tissue that is present in horses or by subclinical peribronchial fibrosis.2,3 The presence of this mild bronchointerstitial lung pattern means that many times the correlation between radiographic changes and clinical disease is poor. Therefore, mild radiographic changes should be interpreted with caution (Fig. 34-7).2,8,8 Objective criteria for assessing heart size have not been established in horses.10 The caudal border of the heart should be straight and should parallel the angle of the ribs. Elevation of the trachea and increased sternal or diaphragmatic contact are indicative of cardiomegaly.10 Assessment of cardiac size is easiest if the entire cardiac silhouette is visible in one image acquired with the x-ray beam centered over the heart. In foals, the cardiac silhouette occupies a larger volume of the thoracic cavity than it does in adults.5 Based on objective measurements of cardiac size in foals, the height should be 6.6 to 7.8 times the length of a midthoracic vertebral body, and the width should be 5.6 to 6.3 times the width of a midthoracic vertebral body.4 Echocardiography is superior to radiography in assessing cardiac size and function. Fluoroscopy, is useful to evaluate esophageal disease, tracheal collapse, and the motion of thoracic masses, but, unfortunately, fluoroscopy configured for equine evaluation is not available readily.10,11 The use of ultrasound has become common in equine practice. Air prevents the transmission of ultrasound waves, so the ultrasound appearance of the normal lung is a bright interface with reverberation artifact characterized by equally spaced lines that parallel the surface of the lung (Fig. 34-8).12 In real time, the normal lung slides along the body wall during respiration. Ultrasound is more sensitive than radiographs in the detection of small pulmonary lesions as long as they extend to the pleural surface.13 Ultrasound is the diagnostic test of choice for evaluating pleural disease in the horse because it is more sensitive to the detection of small amounts of fluid and provides information on the character of the fluid.11,14,14 Ultrasound can also be used to assess the surface of the lung. A few areas of rough pleural surfaces that create a comet tail artifact can be seen in the ventral portions of the normal lung, but more extensive lesions will be present in horses with viral pneumonia and chronic pleural fibrosis (Fig. 34-9).16,17 Ultrasound is an inexpensive and accessible diagnostic test for serial examinations to assess for resolution or progression of disease. Nuclear scintigraphy can provide physiologic information about perfusion and ventilation of the lungs. Ventilation studies can be useful in assessing chronic obstructive pulmonary disease and exercise-induced pulmonary hemorrhage.18,19 The images are characterized by a patchy distribution with hot spots centrally caused by deposition of the injected isotope in the larger airways and cold spots peripherally from lack of ventilation. Additionally, radiopharmaceutical is cleared more rapidly from the lung of horses with chronic obstructive pulmonary disease than in normal horses.20 Perfusion studies are used to evaluate for pulmonary thromboembolic disease, chronic obstructive pulmonary disease, and other diffuse diseases. In combination with ventilation studies, the patient can be evaluated for ventilation and perfusion mismatches. Because of the expensive equipment and need to isolate the patient for approximately 24 hours after the study to allow for radioactive decay, these imaging studies are usually limited to referral hospitals. Computed tomography (CT) is an excellent imaging modality for assessment of the thorax, but because of equipment size its use is restricted to small foals.21 Radiographs complement a physical examination; they do not replace it. Physical examination can be unremarkable, and yet substantial radiographic abnormality can be present. Additionally, the radiographic resolution of disease often lags behind the clinical resolution. This should be considered when evaluating serial studies.22 The patterns of pulmonary disease have been discussed in Chapter 33. As in the dog and cat, the radiographic pulmonary pattern correlates poorly with the location of the disease histologically, diminishing the usefulness of the pattern recognition system. For example, in equine parasitic pneumonia, the most common pulmonary pattern is interstitial, but grossly, the disease is predominantly alveolar, and horses with a diffuse interstitial lung pattern have peribronchial disease on histologic examination.2,23 But radiographic patterns can reflect the severity of the disease with bronchial and interstitial patterns suggesting less-severe disease than an alveolar pattern.22 The distribution of the pulmonary disease may be more useful with regard to the cause of the pulmonary disease than the pattern itself.5,24 For example, bronchopneumonia and aspiration pneumonia tend to have a cranioventral and caudoventral distribution, whereas pulmonary edema and interstitial pneumonia are more caudodorsal to diffuse in their distribution. Inhalation and aspiration pneumonia in the adult horse and foal appear similar to pneumonia in other species. In adults, bronchopneumonia is usually a result of transportation or stress, whereas in foals it is usually caused by sepsis or aspiration.25,26 In adults and foals, bronchopneumonia can occur secondary to viral pneumonia.26 Bacterial pneumonia usually occurs in the cranioventral and caudoventral portions of the lung.27 Although it is present in the lung fields cranial to the heart, this region is difficult to evaluate radiographically, so the disease is most conspicuous when superimposed on the caudal border of the heart (Fig. 34-10). Bacterial pneumonia can result in an interstitial or alveolar lung pattern depending on the severity (Fig. 34-11).23 Abscess formation is seen in 10% to 15% of horses with pneumonia (Fig. 34-12).23 The ultrasonographic appearance of pneumonic lung is a uniform soft tissue echogenicity that resembles the appearance of liver (Fig. 34-13). Air-filled bronchi appear as hyperechoic, linear, branching structures that have a reverberation artifact. Fluid-filled bronchi appear as anechoic branching tubes (Fig. 34-14). Fluid-filled bronchi can be differentiated from blood vessels with Doppler interrogation. Interstitial pneumonia occurs in foals and adults and can be acute or chronic.28,29 The causative agent is usually not identified but may include infectious agents, toxins, systemic inflammatory response syndrome, or allergic factors.22,25,28–30 Interstitial pneumonia in foals is usually acute, and affected foals are typically 6 weeks to 6 months of age.28,31 Chronic interstitial pneumonia has a more favorable prognosis, whereas acute interstitial pneumonia has a high mortality rate.29,32 Whether the disease is acute or chronic, the radiographic changes are the same, a diffuse interstitial lung pattern.28,31 A mild to moderate bronchial lung pattern may also be present.29 The disease can result in increased vascular permeability and secondary pulmonary edema.32 The severity of the changes on the initial radiographs and progression of the changes on subsequent radiographs are negative prognostic indicators.22 Interstitial pneumonia is rare in adults, and because the lung has a limited range of responses to injury, it usually presents as a chronic problem with secondary fibrosis, and affected horses usually respond poorly to treatment.26,30,32–34 The most common radiographic appearance is a patchy to diffuse alveolar lung pattern.28 Recently, a specific form of multinodular interstitial pneumonia thought to be secondary to equine herpesvirus type 5 (EHV-5) has been reported.33,35 Clinical signs include weight loss, fever, tachypnea, tachycardia, neutrophilic lymphocytosis and hyperfibrinogenemia, and increased respiratory effort. Imaging findings are severe multifocal nodules of 1 to 5 cm in diameter that are evident radiographically and with thoracic ultrasound.33,36 Other causes of a diffuse interstitial to military nodular lung pattern are the eosinophilic pneumonopathy, including multisystemic eosinophilic epitheliotropic disease (systemic disease) and idiopathic chronic eosinophilic pneumonia (localized pulmonary disease) and pulmonary silicosis.37–40 Pneumonia caused by Rhodococcus equi in foals is a specific disease entity that frequently has a different radiographic appearance than bronchopneumonia or interstitial pneumonia. Rhodococcus equi pneumonia typically has a patchy to diffuse alveolar lung pattern and/or discrete pulmonary nodules (abscesses) (Fig. 34-15).8,25,41,42 It can also result in consolidation of one lung lobe.43 Radiographic changes are most apparent at approximately 3 weeks after infection.43 The severity of the radiographic changes has been negatively associated with prognosis.44 Foals with an extensive alveolar lung pattern or pulmonary nodules (abscesses) were more likely to die.42 Tracheobronchial and cranial mediastinal lymphadenopathy can also be detected.42 In most foals, the radiographic signs resolve completely within 3 months of appropriate therapy.8,43 Ultrasonographic evidence of pneumonia has been highly associated with radiographic abnormalities and may be a useful diagnostic field test.45 Ultrasound may also allow the detection of abscesses within consolidated lung lobes that are not evident radiographically (Fig. 34-16). Up to 74% of foals have R. equi infection in at least 1 additional extrapulmonary site, including gastrointestinal tract, abdominal lymphadenopathy, abdominal abscess, uveitis, synovitis, and pyogranulomatous hepatitis. A thorough physical examination and abdominal ultrasound examination are indicated in these patients to determine the extent of the disease because the prognosis is reduced significantly in foals with concurrent extrapulmonary disease.46 Fungal pneumonia is rare in horses. It has a wide range of radiographic appearances. Although it cannot be differentiated reliably from bacterial pneumonia on the basis of radiographic appearance, the distribution of fungal pneumonia is usually more diffuse than bacterial pneumonia and typically has an interstitial to indistinct nodular appearance.23,47–50 Tracheobronchial lymphadenopathy and pleural effusion may also be present.47,49 Viral pneumonia itself does not usually result in radiographic changes, but radiographs can still be indicated to evaluate for concurrent bacterial pneumonia, which is common and results in more severe clinical disease.16,23,23 Ultrasonographically, there may be roughening of the pleural surface with production of comet tail artifacts and consolidation of the cranioventral aspect of the lung within 5 to 10 days of infection.16 Pulmonary abscesses can form as a result of pleuropneumonia or develop independently and predominantly affect foals younger than 6 months of age.52,53 They can occur anywhere in the lung, but unlike bronchopneumonia, abscesses are most commonly detected in the caudodorsal lung field.14,54 This may be because of the excellent contrast provided by air-filled lung in this region. Abscesses are discrete, focal, soft tissue nodules or masses that may be sharply or poorly margined. If the abscess communicates with a bronchus or contains gas-forming bacteria, a discrete gas-fluid interface will be seen on horizontal-beam radiographs (Fig. 34-17). Well-margined pulmonary consolidation can mimic the appearance of a pulmonary abscess.
The Equine Thorax
Radiographic Technique
Normal Anatomy
Craniodorsal Projection
Caudodorsal Projection
Caudoventral Projection
Cranioventral Projection
Foals
Adults
Heart
Alternative Imaging Modalities
Pulmonary Disease
Pneumonia
Pulmonary Abscess
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The Equine Thorax