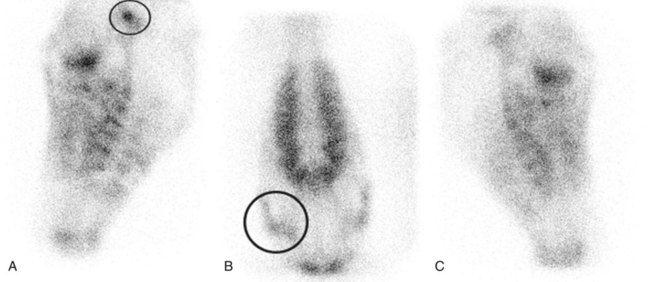
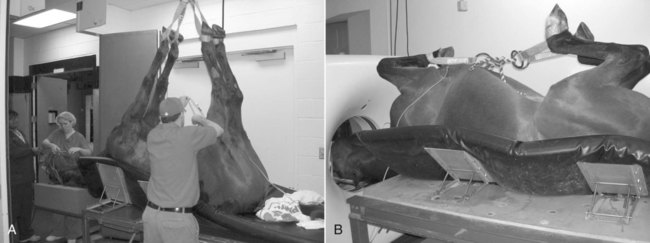
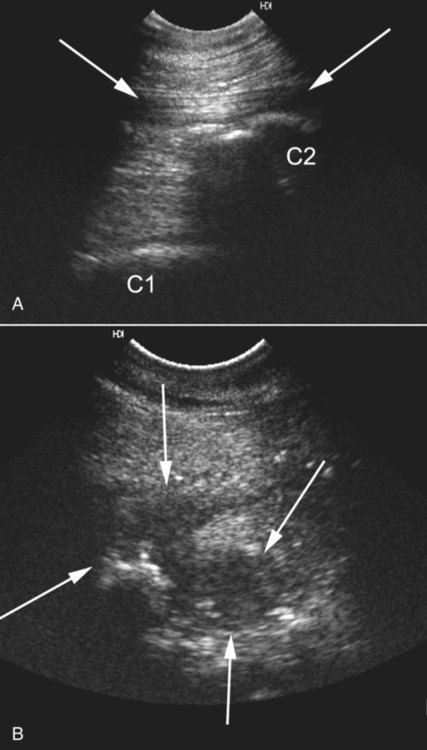
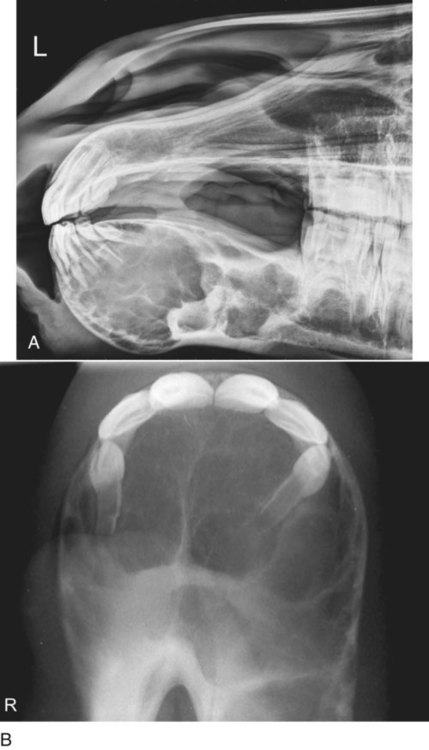
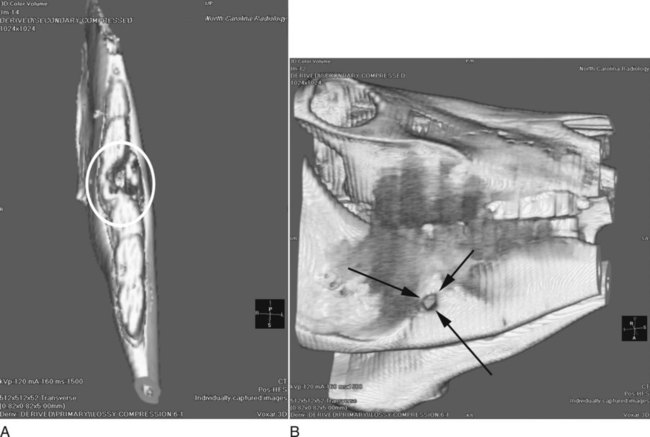
In the last several years, there has been increased use of cross-sectional imaging modalities such as computed tomography (CT), magnetic resonance (MR) imaging, and ultrasound for imaging the equine head. This has simplified identification of morphologic abnormalities. In addition, postprocessing programs allowing multiplanar and three-dimensional reconstruction of CT and MR images have augmented surgical planning.1,2 Despite the enhanced capabilities provided by CT, MR imaging, and ultrasound, conventional radiography is still the main modality used to evaluate the equine head.3–6 The large gas-filled structures of the equine head, such as the guttural pouches, larynx, pharynx, nasal cavity, and paranasal sinuses, enable diagnostic-quality radiographs to be obtained with portable radiographic units. The main limitation of radiography is the superimposition of multiple complex structures. Despite the difficulties associated with interpretation of conventional equine skull radiographs, they are helpful in providing diagnostic information in a majority of diseases that occur in the head, although the true extent of the disease may be underestimated.7 Subsequently, other techniques can be used to provide more detailed or specific information after identification with radiography. Scintigraphy has been applied primarily to localize sites of bone remodeling. Bone-seeking radiopharmaceuticals, such as technetium-99 m methylene diphosphonate, bind to hydroxyapatite crystals in regions of osteoblastic activity. In the head, the main use for nuclear medicine is evaluating dental disease and differentiating sinusitis of dental origin from other causes.8 This can be particularly difficult radiographically because lesions of the teeth may not be detected as a result of superimposition of normal structures or disease or the presence of only minimal bone lysis. In addition, scintigraphy is also useful for identifying regions of bone remodeling caused by degenerative joint disease within the temporomandibular and temporohyoid joints, which may not be evident on radiographs (Fig. 10-1). Radioactive labeling of white blood cells has also been used in the evaluation of tooth abnormalities. However, the overall low level of radioactivity in sites of abnormal white cell accumulation causes poor resolution and does not provide adequate landmarks, making this technique inaccurate.9 Overall, the primary limitation of scintigraphy is poor spatial resolution. Thus, nuclear medicine has a high sensitivity for detection of bone destruction and remodeling, although scintigraphy is not as specific in detecting the cause of remodeling compared with radiography.9 The sensitivity of conventional radiography for equine dental disease is only approximately 50%,9–11 but when used in combination with scintigraphy the sensitivity increases to 97.7% and the specificity to 100%.9 The use of cross-sectional imaging eliminates the problem of overlying structures. CT and MR imaging allow the evaluation of transverse slices of the head that are generally 0.5 mm to 1 cm thick. These images provide good anatomic localization (Fig. 10-2). In addition, three-dimensional reconstructions of CT images can be generated that can aid in surgical planning and visualizing lesions not easily identified on transverse images (Fig. 10-3). CT and MR imaging require specialized equipment, including custom tables and hoists (Fig. 10-4) and a purpose-built room to accommodate the size of the horse. Standing CT units are available in Europe but to date are not present in the United States. These standing units are divided into mobile CT or fixed CT units. With a mobile CT unit, the CT scanner is placed on rails, and the horse is sedated and stands with its head in the CT scanner. Instead of the table moving through the gantry, the gantry moves while the table remains still. The fixed CT unit is a standard CT unit, and the horse is sedated and the head placed on the CT table. The horse is standing in a specially made stock, and the floor has numerous air jets that allow the stocks and horse to float above the floor. This allows the table to move through the gantry with minimal resistance. Many sources provide CT and MR imaging of normal anatomy.12–14 Ultrasonography has been used to evaluate skull fractures as well as temporomandibular joints, retrobulbar masses, and jugular vein thrombosis.15 Ultrasonography is also useful for evaluation of the superficial soft tissue structures of the head, with the major limitations being the contour of the head, which prevents adequate transducer-skin contact, and the inability of sound to penetrate bone. The most useful application of ultrasound is evaluating soft tissue structures where the bone is not obstructing the region of interest, such as in the guttural pouches to look for fluid, and allowing the evaluation of draining tracts associated with atlantoaxial septic bursitis (Fig. 10-5). Ultrasound can also help evaluate the size and appearance of lymph nodes in horses afflicted with Streptococcus equi. In addition, the use of ultrasound has been suggested as an aid in the evaluation of the larynx.16 The rostral aspect of the head is the area rostral to the premolar teeth. The standard radiographic projections to evaluate this region include a lateral and a dorsoventral projection. Intraoral radiographs are useful to eliminate superimposition of structures and are accomplished by placing a plastic bag over a radiographic cassette and then inserting the cassette into the mouth (Fig. 10-6). A dorsoventral projection is used to evaluate the incisive bone, and a ventrodorsal projection allows assessment of the rostral aspect of the mandible. Diseases that involve the rostral equine head include fractures, neoplasia, and cyst formation.3,4,4 Fractures generally occur in young, inquisitive animals that become startled while chewing or playing with a fixed object.6 This causes a displaced fracture involving the incisive teeth with extension into the diastema, which is the portion of the body of the mandible or maxilla without teeth. These fractures are usually moderately displaced and identified easily. However, radiographs tend to underestimate the extent of incomplete fracture lines that may extend into the mandible or involve premolar tooth roots. Involvement of tooth roots by the fracture increases the complications of surgical repair because of the increased likelihood of tooth root infection and abscess formation. Tumors that occur on the rostral head are rare and generally benign. Osteoma is a benign tumor that can affect the mandible, maxilla, paranasal sinuses, and nasal cavity. The main feature of an osteoma is that it has an intense, well-demarcated mineral opacity and is usually midline in the rostral mandible.4 Adamantinomas, also known as epidermoid cysts, cause a unilateral enlargement of the rostral mandible or ventral aspect of the body of the mandible in young animals.3,4,4 This lesion is an expansile mass that can look clinically similar to osteosarcoma.3 Another cause of cystlike enlargement and septation in the mandible of a young horse is nutritional hyperparathyroidism.3 Large aneurismal bone cysts are also possible in the rostral mandible of a young horse (Fig. 10-7). Soft tissue tumors have also been described as expansile lesions that cause bone lysis and displace the incisor teeth but generally consist of a large soft tissue mass with secondary bone involvement.17 Either mandible is difficult to examine in its entirety because of superimposition of the contralateral mandible and parts of the skull. Evaluation of the temporomandibular joints and the rami of the mandible requires oblique radiographs, CT imaging, or MR imaging. Standard radiographic views for the mandible include lateral, dorsoventral, and two oblique projections. The goal of an oblique radiograph is to allow the ramus or body of each mandible to be evaluated individually.4,6 Thus right 45-degree dorsal-left ventral oblique (RDLVO) and left 45-degree dorsal-right ventral oblique (LDRVO) radiographs should be obtained. When obtaining oblique radiographs, care should be taken to place the appropriate radiographic marker to identify the image; this is discussed in detail in Chapter 7. Radiographs of the mandible are usually performed to evaluate the mandibular tooth roots or the mandibular body for fractures. Mandibular tooth root infections are suspected when swelling is present in the mandibular region that frequently manifests itself as a sinus tract draining from the ventral aspect of the ramus.6 Evaluation of the extent of this tract can be performed by a metallic probe or injection of contrast medium. This contrast-medium procedure is performed while obtaining an oblique radiograph to isolate the involved area of the mandible further while eliminating superimposition. The goal of adding the contrast medium or metallic probe is to trace the sinus tract to the source of the infection, which often centers on the apical aspect of the infected tooth root. The radiographic findings of apical tooth root abscesses include indistinct margins of the lamina dura, loss of the normal outline of the tooth root, blunting of the tooth root, widening of the periodontal membrane, and frequently an associated lytic tract extending out of the ventral cortex of the mandible (Figs. 10-8 and 10-9).4,6 In chronic infections, the mandible may have a periosteal reaction associated with the defect and extension of the infection into the soft tissues. Bone formation can extend on the medial and lateral borders of the mandible, obscuring the mandible and causing a loss of detail on the radiographs because of superimposition.6 Fractures of the caudal aspect of the mandible may be unilateral or bilateral. Because of the superimposition of the teeth, mandibular fractures are difficult to evaluate without the use of oblique radiographic projections.4,6 Caudal mandibular fractures are usually incomplete and have a worse prognosis if the fracture line involves a tooth root that may lead to a tooth root infection.4 Dorsoventral radiographs can be acquired in the standing horse, but care needs to be used because the x-ray tube is difficult to move out of the way rapidly if the horse becomes startled; this could cause injury to personnel, equipment, and the patient.18 Recently, more emphasis has been placed on the ultrasonographic appearance of the temporomandibular joint, including the normal appearance.19 After comparing radiography, scintigraphy, and ultrasound to diagnose temporomandibular arthropathy in a horse, ultrasound was considered the least expensive, technically easiest, and most informative.20 However, sonography is useful for this purpose only if applied by trained sonographers. CT and MR imaging are useful to assess the mandible and temporomandibular joint. In terms of assessing tooth root abscesses, the same changes described with radiography can be identified with CT; however, CT is also able to assess whether fragmentation or lucencies within the tooth are present (see Fig. 10-2).1 In addition, CT can better evaluate mandibular fractures and allow detection of subtle fracture lines obscured by superimposition on conventional radiographs. For the temporomandibular joint, both CT and MR imaging allow evaluation of the surrounding soft tissues for evidence of infection or swelling, determine if the joint is misaligned, and identify bone lysis associated with the mandibular condyle or mandibular fossa. Because horses are obligate nasal breathers, the nasal cavity and paranasal sinuses are very large to provide adequate airflow during exercise. The extensive sinus system occupies the majority of the head and has an intricate communication system within the sinuses as well as in the nasal cavity (Fig. 10-10). On each side of the horse are frontal, caudal maxillary, rostral maxillary, and sphenopalatine sinuses. The unique characteristics of this sinus system is that among domestic species the horse is the only species in which the frontal sinus communicates indirectly with the nasal cavity through the caudal maxillary sinus; in other species the communication is direct.21 The frontal sinus, more correctly the conchofrontal sinus, is in the caudodorsal aspect of the head and overlies the rostral portion of the calvaria, medial to the orbits and extending rostrally as the closed portion of the dorsal concha. The frontomaxillary opening on the rostrolateral aspect of the conchofrontal sinus allows communication between the conchofrontal and caudal maxillary sinuses. The caudal maxillary sinus and the rostral maxillary sinus are in the lateral aspect of the caudal head and overlie the maxillary cheek teeth. These two sinuses are divided by an oblique septum that varies in position. Both sinuses communicate with the nasal cavity by a small, shared communication nasomaxillary opening that extends to the middle nasal meatus.21 This opening bifurcates to allow communication with the rostral and caudal maxillary sinuses while preventing direct communication between the two maxillary sinuses.22 The sphenopalatine sinus communicates rostrally with the caudal maxillary sinus and infrequently has direct communication with the ventral nasal meatus.22 This sinus is located ventral to the cranial vault within the sphenoid bone, and the lateral wall is associated with the pterygoid fossa. The septum between the right and left sides of the sphenoid varies in position, and the two sides are never equal size.22 The sphenopalatine sinus is associated closely with the ethmoid labyrinth and optic canal; therefore disease such as infection or ethmoid hematomas can result in vision loss. For radiography of the nasal cavity and paranasal sinuses, the acquisition of left to right and right to left lateral radiographs is important, as well as dorsoventral, left ventral, right dorsal oblique (LVRDO) and LDRVO radiographs, to maximize the chance of detecting abnormalities such as fluid lines and determine if bilateral disease is present.23 When performing oblique radiographic projections, the angle should be approximately 60 degrees in the dorsal or ventral direction to try to minimize the superimposition of the contralateral sinus.4 The oblique radiographs can also be acquired with a speculum placed within the horse’s mouth so that the occlusive surface of the teeth can be better evaluated.24
The Equine Head
Radiography Versus Other Imaging Modalities
Abnormalities of the Equine Head
Rostral Head (Incisive Region and Rostral Mandible)
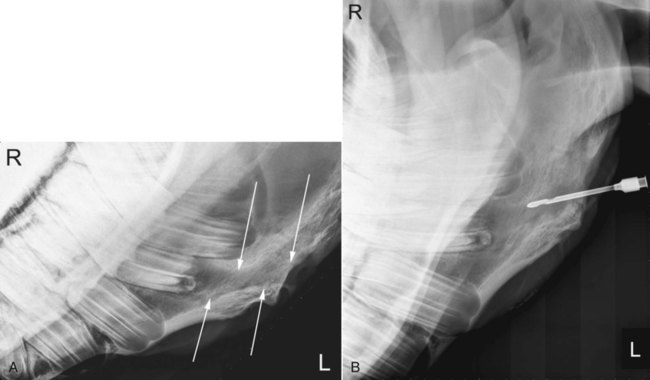
Mandible
Nasal Cavity, Paranasal Sinuses
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The Equine Head