CHAPTER 71 The Dilemmas of Cytological Evaluation of the Feline Lymph Node
Cytological examination of tissues is an integral part of the veterinary diagnostic repertoire in cats. Practically any tissue of the body, including peripheral and internal lymph nodes, is amenable to direct or ultrasound-guided fine-needle aspiration. Studies in dogs and cats have evaluated the sensitivity and specificity of cytological evaluation of various tissues compared with histopathology, and for the assessment of metastasis to lymph nodes.1–3 Remarkably, these studies have shown that in lymph nodes, cytopathology correlates well to histopathology about 50 per cent of the time, and is highly sensitive (100 per cent) and specific (96 per cent) for detecting metastasis.1,2 The most important challenge associated with cytological evaluation of feline lymph nodes is to differentiate the normal changes from the various abnormal processes involving these tissues, and to identify specific diseases. This chapter will illustrate a systematic approach for resolving the cytological dilemmas of lymph node evaluation in cats.
SAMPLE ACQUISITION AND SMEAR PREPARATION OF LYMPH NODES
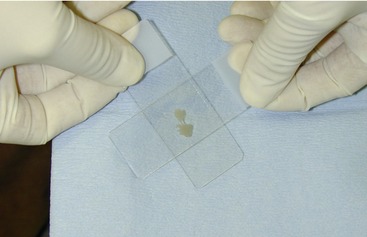
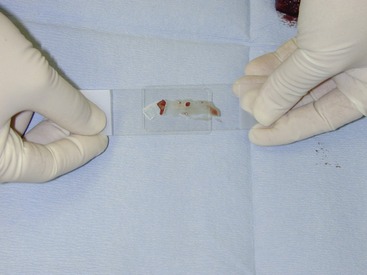
Veterinarians can perform fine-needle aspiration of enlarged lymph nodes routinely in cats, similar to dogs. Proper sample acquisition and smear preparation are just as important to the overall cytological interpretation of lymph node samples as the microscopic evaluation, because inferior collection and preparation techniques often lead to poor cellular preservation of the notoriously fragile lymphocyte.4–6 Fine-needle core or “stab” technique samples often are superior to fine-needle “aspiration” techniques in terms of cellular integrity during the collection process.6 Gentle vertical pull-apart “squash smears” (Figure 71-1) or “blood smear” methods provide the best morphological preservation of lymphocytes.6 Horizontal pull-apart smears (Figure 71-2) should be avoided, because they often induce lysis of lymphocytes (Figure 71-3).6
Samples typically are stained with rapid Romanowsky-type cytological stains, such as Diff-Quick, Wright’s, or a modified Wright’s stain.6,7 Unstained samples that are shipped to a diagnostic laboratory should be submitted separately from any formalin-fixed tissues, because exposure to either formalin or the formalin fumes causes an excessively blue-staining, nondiagnostic sample.6,8 A good practice for veterinarians to employ, even if they are skilled cytologists, is to send similar slides to a pathologist to verify the cytological diagnosis. Likewise, histological examination of tissues remains the gold standard for definitive diagnosis.
NORMAL LYMPH NODE CYTOLOGY
The initial challenge in lymph node cytology is to determine if the sample is normal or abnormal. In reality this can be a challenging task, particularly with feline lymph nodes because what constitutes normal lymph node cytology is somewhat dependent on the location of the node. For example, normal mesenteric lymph nodes may have a higher percentage of immature lymphocytes and plasma cells compared with their normal peripheral counterparts.7,8 This difference is hypothesized to occur because mesenteric lymph nodes are exposed to larger numbers of antigens derived from the intestinal tract compared with peripheral lymph nodes.7,8
Small lymphocytes in most normal peripheral lymph node cytology samples represent approximately 85 to 90 per cent of the entire lymphocyte population.6–9 Likewise, immature lymphocytes typically compose the remaining 10 to 15 per cent of the population. Immature lymphocytes are large or medium-sized cells, or a combination of both. Small numbers of plasma cells, macrophages, neutrophils, eosinophils, and mast cells also are seen in cytology samples from normal lymph nodes, but each should represent less than 1 per cent of the entire nucleated cell population.6–8,10,11
ABNORMAL LYMPH NODE CYTOLOGY: THE INITIAL DILEMMA
Lymphadenopathy is defined as an enlargement of one or more lymph nodes. When multiple lymph nodes are enlarged throughout the body, the designation of generalized lymphadenopathy is used. Generalized lymphadenopathy is recognized in cats, but this finding is certainly more common in dogs.7 Causes of generalized lymphadenopathy in cats include infectious diseases such as feline immunodeficiency virus (FIV) and feline leukemia virus (FeLV), systemic bacterial or fungal infections, lymphoma, and dermatopathic conditions.12–19 Three references are reported documenting unusual generalized lymphadenopathy in cats: one detailing a distinctive peripheral lymphadenopathy resembling lymphoma in six cats, five of whom subsequently resolved; one describing peripheral lymph node hyperplasia in young cats; and one attributing lymphadenopathy to methimazole treatment for hyperthyroidism.20–22 Latter portions of this chapter will discuss changes in lymph nodes associated with some of these diseases. Enlargement of solitary lymph nodes is a relatively common occurrence in cats, as is mesenteric lymphadenopathy, which is more difficult to detect clinically. Accordingly, it is extremely important for clinicians to be able to palpate enlarged peripheral lymph nodes for collection of quality cytological samples. Ultrasound-guided aspiration of lymph nodes generally is recommended for mesenteric or mediastinal lymphadenopathy.
Feline lymph nodes typically are quite small, so palpable lymphadenopathy should be considered an abnormal clinical finding. However, it is important for the clinician to remember that palpable changes in lymph node size are not sufficient for a definitive diagnosis; cytological or histopathological examinations are required. Additionally, minimal enlargement of a lymph node does not exclude the potential for disease within the node. One study in dogs and cats evaluated the predictability of determining metastatic disease based on palpable lymph node enlargement compared with histopathological and cytopathological examinations.2 The results of this study showed there is relatively good sensitivity (93 per cent) but poor specificity (14 per cent) using lymph node palpation alone when the lymph nodes are significantly enlarged.2 However, when lymph nodes are only mildly increased in size, the sensitivity for metastasis based on palpation alone decreased substantially (60 per cent).2 In contrast, cytopathology compares relatively well to histopathology, and cytological evaluation of lymph nodes is recommended for assessing lymph nodes for metastatic disease.2
THE REACTIVE HYPERPLASTIC LYMPH NODE DILEMMA
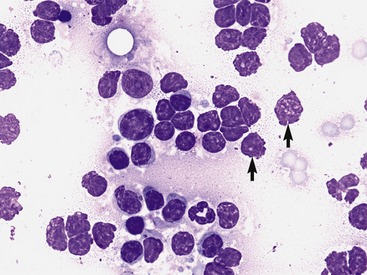
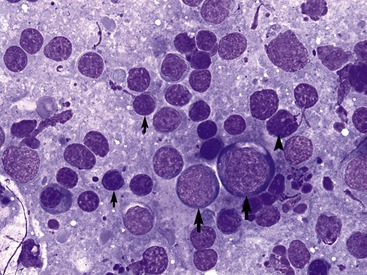
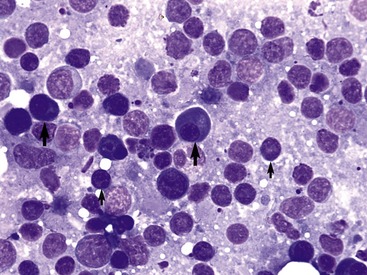
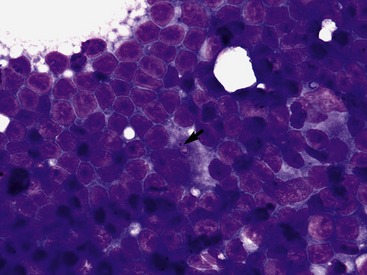
By definition, hyperplastic lymph nodes have increased numbers of lymphocytes, generally reflecting an increased number of immature lymphocytes within the tissue.6,8 Although some veterinarians use this term synonymously with “reactive” lymph nodes, reactive lymph nodes typically imply increased numbers of plasma cells within the node. These two processes often are commingled within the same lymph node, leading some clinicians to use the two terms interchangeably. The percentage of immature lymphocytes in a hyperplastic lymph node is increased compared with normal lymph nodes, varying from 15 to 20 per cent to approximately 35 to 40 per cent (Figure 71-4) in marked hyperplasia.6,8 Higher percentages of immature lymphocytes raise a strong suspicion for lymphoma. Plasma cell numbers also are usually increased, often representing greater than 5 per cent of the total nucleated cell population within the lymph node (Figure 71-5). Extremely high percentages of plasma cells (>50 per cent) in a lymph node cytological sample may represent an extramedullary plasma cell neoplasm.23–25
A variety of nonspecific disorders are capable of inducing these lymph node changes. Antigenic stimulation, although a vague and nonspecific term, is thought to stimulate these changes in the lymph nodes. Lymph nodes filter and process antigens, so exposure to new or excessive amounts of these antigens can lead to proliferation of lymphocytes and production of antibodies by plasma cells.6–8 Many infectious, inflammatory, allergic, and neoplastic disorders are capable of eliciting this type of response. This response is nonspecific and an etiology often is not identified in the cytological sample. However, thorough microscopic examination for potential causes of reactive hyperplasia, such as metastatic neoplasia and inflammation from infectious diseases, is recommended when reactive hyperplasia is evident cytologically. Specific types of neoplasia and infectious diseases common to cats will be discussed in later sections of this chapter.
THE INFLAMMATORY LYMPH NODE DILEMMA
Increased numbers of inflammatory cells in a lymph node cytological sample are abnormal, but it is often difficult to differentiate a true lymphadenitis from the presence of inflammatory cells resulting from drainage of a regional inflammatory site. Reactive hyperplasia frequently is present in addition to the inflammatory infiltrate. The inflammatory cells are neutrophils most commonly, but macrophages, multinucleated giant cells, eosinophils, or a combination of these cells often are present. Mast cells also are present occasionally as a component of inflammation, but if these cells are present in larger numbers, they may represent disseminated mast cell disease.26,27 Basophils are seen rarely in peripheral tissues and lymph nodes.
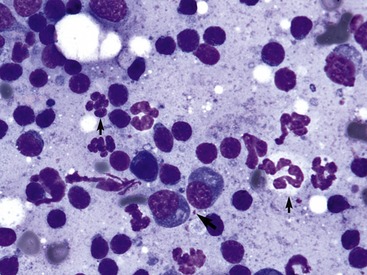
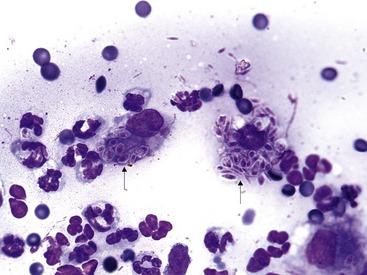
Increased neutrophils in a lymph node cytological sample indicates suppurative lymphadenitis, or as mentioned previously, drainage of suppurative inflammation distal to the node. If neutrophil numbers are increased considerably and multiple lymph nodes are involved, infectious etiologies are most likely (Figure 71-6). Bartonella henselae (bartonellosis, cat scratch disease), Francisella tularensis (tularemia), and Yersinia pestis (Pasteurella pestis, plague) are known causes of suppurative inflammation within multiple lymph nodes in cats.17,28–31 Microscopic identification of any of these specific bacteria in the lymph node cytological sample is rare. Therefore culture and sensitivity testing and molecular-based tests such as polymerase chain reaction (PCR) for specific microorganisms often are required for identification of the causative agent. Early in the disease course of systemic or local fungal diseases, neutrophilic infiltration into lymph nodes also may occur. However, with time, the inflammatory component will change from suppurative to a mixed population of inflammatory cells. Neutrophilic infiltrates in feline lymph nodes also is seen with metastatic neoplasia, especially squamous cell carcinoma (Figure 71-7). The inflammation often is confined to regional draining lymph nodes, so generalized lymphadenopathy usually is not present.
Pyogranulomatous lymphadenitis is a relative uncommon finding in feline lymph node cytological samples. Neutrophils, macrophages, and occasional multinucleated giant cells typically comprise this type of inflammation. Eosinophils also are seen occasionally with pyogranulomatous inflammation. Some clinical pathologists choose to use the term mixed-cell inflammation interchangeably with pyogranulomatous inflammation, and if a neutrophilic component is absent, the designation of granulomatous inflammation is appropriate. The main components of this type of inflammation are macrophages and giant cells, which suggest a more insidious type of inflammatory process within the lymph node. In cats, fungal and certain bacterial diseases are the primary causes for this type of inflammation, but feline infectious peritonitis (FIP) is known to cause a similar inflammatory infiltrate in lymph nodes.32,33
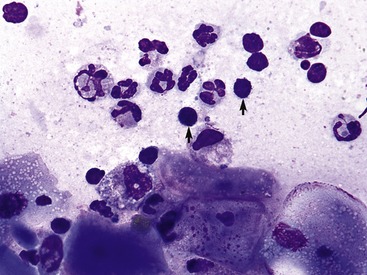
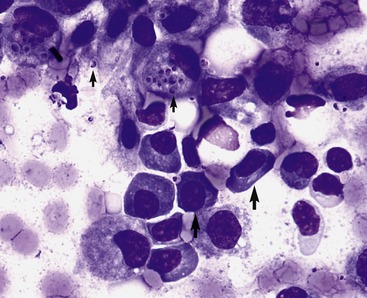
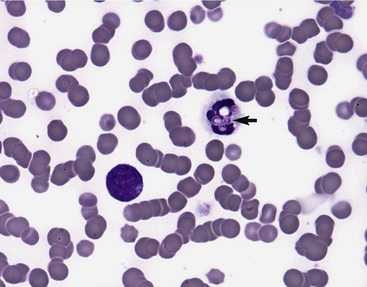
One of the most common systemic fungal diseases responsible for lymphadenopathy in cats is histoplasmosis.19 Histoplasma capsulatum infection often presents with systemic disease, including lymphadenopathy, so the clinical history, physical examination findings, and other diagnostic evidence of disseminated disease also are paramount for the diagnosis.19 Although peripheral lymph nodes are easier to sample if enlarged, mesenteric lymph nodes often are a good source for detecting histoplasmosis, especially if gastrointestinal signs are present. Cytological examination of lymph nodes from cats with histoplasmosis often reveals reactive hyperplasia, but increased numbers of macrophages, occasional multinucleated giant cells, and neutrophils often are present.19,34 Careful microscopic examination for the yeast of H. capsulatum is indicated if these inflammatory cells are noted and histoplasmosis is on the list of differential diagnoses. The yeast are approximately 2 to 4 µm in diameter, have a round to oval shape and a thin nonstaining capsule with a round to comma-shaped blue-staining nucleus (Figure 71-8).19 Budding yeasts are identified occasionally (Figure 71-9). The organisms often are found both within inflammatory cells and free in the background of the smears. In a related finding, H. capsulatum also is identified occasionally in leukocytes found in peripheral blood smears (Figure 71-10).19,34–36 Additionally, several diagnostic tests, including a specific test for H. capsulatum cell-wall polysaccharide antigen (performed preferably with urine), are available to aid in the diagnosis of histoplasmosis.37–39
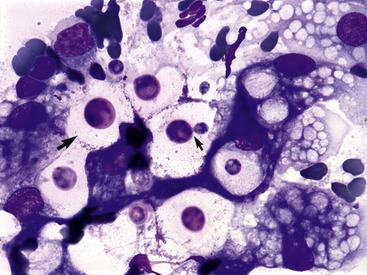
Cryptococcus neoformans is another fungal organism capable of inducing lymphadenopathy in cats.36,40 The lymphadenopathy generally is confined to the head and neck because the primary disease usually is located in the nasal cavity and sinuses (Figure 71-11). While organisms may be identified in nasal discharge, lymph nodes also are a readily available source for possible identification of this fungus. Like histoplasmosis, the inflammatory component within the lymph node often is pyogranulomatous, but eosinophils also may be present. Similarly, the node often is reactive and hyperplastic. The yeast of C. neoformans is more variable in size compared with H. capsulatum, ranging from 5 to 30 µm in diameter including the polysaccharide capsule.40 It usually has a large nonstaining capsule, although acapsular forms are reported, and is characterized by narrow-based budding (Figure 71-12).37,41 The cryptococcal antigen latex agglutination test also is available for aiding in the diagnosis of this fungal disease. 37,40–42

Sporothrix schenckii, the cause of cutaneous sporotrichosis, is another fungal organism that is involved occasionally in regional lymphadenopathy in cats.36,43 Initial cutaneous lesions often are similar in appearance to cat-bite abscesses, and are characterized by draining tracts that do not respond to antibiotic therapy. Cytological evaluation of these lesions varies from suppurative to pyogranulomatous inflammation, with affected draining lymph nodes sharing similar cytological features in addition to reactive hyperplasia. The yeasts are somewhat similar in appearance to H. capsulatum, but are slightly larger in size, and have round but also elongated or “cigar-shape” nuclei in addition to the nonstaining thin capsule (Figure 71-13).38 Other fungal diseases, such as blastomycosis and coccidioidomycosis, are reported in cats, but are less common.36
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


