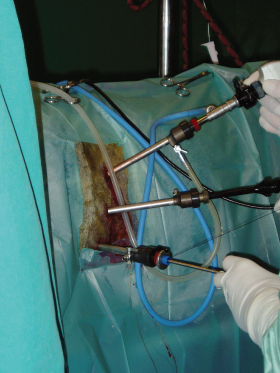
Ideally, this requires placing the camera portal between the two instrument portals. This is possible in the recumbent horse but is more challenging in the standing horse where the surgeon may be disturbed by the assistant holding the scope. For this reason, the laparoscope is often positioned dorsally to the instrument portals in the standing horse (Figure 3.2). The surgeon should take advantage of the laparoscope’s magnification ability by using close-up views when actually placing the sutures. When instruments or sutures are moving away from the target tissue, a backward movement of the scope allows an overall view of the surgical area and allows the surgeon to redirect his instruments. This backward movement is also very useful to give a three-dimensional image, especially to assess good positioning of the needle into the needle holder. For an intracorporeal knot, a wide-angle shot makes the procedure easier.
Sutures and knot tying follow all the principles of classical surgery, and a perfect knowledge of the technical properties of the knots is mandatory. Even if specific extracorporeal knots are used in laparoscopy, most of the techniques used in classical surgery may be adapted in laparoscopic surgery.
Some specific words linked to the art of suturing and knot tying are to be learned by the laparoscopic surgeon. There are two basic parts of a suture. The “standing part” of the suture is the bulk of the suture, which includes the segment that may have a needle attached to it, and the “end” of the suture is the short segment that is grasped by the holding forceps after having made the loop around the latter in order to make a knot.
Instrumentation and Suture
Instruments for laparoscopic suturing and knot tying include a needle holder, a grasping forceps that can be a second needle holder, scissors, a knot pusher, trocars and cannula with a reducer cap, sutures, and needles. The needle holders have linear handles to provide a 360° rotation of the instrument and a locking mechanism to securely hold the needle. Curved jaws can facilitate the formation of loops for intracorporeal suturing and to reach, to retrieve a needle from the tissue, and to replace a needle into the needle holder. The size of the needle holder and the holding forceps should be 60 cm long in order to have part of the shaft outside of the abdomen (Figure 3.3). This can facilitate the manipulation of the suture, using the cannula as a pivot point. In our experience, human instruments are too short for most of the procedures in horses and special instruments should be used. Strong jaws are useful in horses where big needles are sometimes used. Scissors with curved jaws are very useful in laparoscopy because they allow a good visualization of the suture threads and the knot. Special knot pushers are available with various shapes and configurations. One of the most useful is that with a small cup at the tip to place the knot and a hole at the middle of the cup exiting laterally at the shaft level. This kind of knot pusher also has a sheath with a sharp end that allows cutting the suture after tying the knot (Figure 3.4). Knot pushers are used to advance an extracorporeal knot or an extracorporeal loop or hitch into the body cavity and tighten it against the tissue. Babcock forceps may also be used to push a knot, but the pressure applied on the knot is sometimes not as strong as when applied using a knot pusher, and they are not widely used in equine laparoscopy.
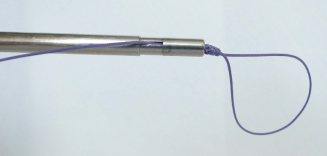
Figure 3.3 Needle holder (60 cm) adapted for equine laparoscopy. The needle holder should be long enough to have part of the shaft outside the abdomen.

Sutures may be introduced into the abdomen through an introducer sleeve that contains a rubber gasket at the external opening to prevent loss of pneumoperitoneum during suturing, especially when a suture thread is kept outside of the abdomen. This is more important in the recumbent horse when the loss of pneumoperitoneum is quick and visualization is rapidly compromised. The gasket should allow an easy way to introduce and to remove the needle from the body cavity. For this reason, the common cannula containing a magnetic valve is not adapted for suturing when a needle is used.
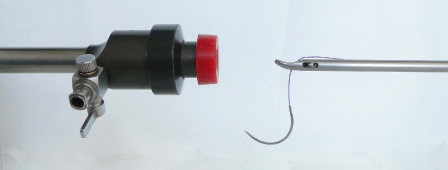
Laparoscopic sutures are available in a wide variety of sizes, materials, and needle configurations. In equine laparoscopy, the size of the needle should be large enough to pass through the tissue and small enough to be introduced through a 10-mm cannula. A half-circle, 36-mm needle, for example, easily fits through a 10-mm-diameter trocar and is large enough to be useful for suturing in the horse. The needle should be introduced with the needle holder grasping the suture 1–2 cm behind the swage of the needle in order to introduce the latter in a longitudinal direction (Figure 3.5). Larger curved needles may be bent into a ski configuration to be passed through a 10-mm-diameter trocar. For a specific procedure such as nephrosplenic space closure, special large trocars (25 mm in diameter) are used. Valves are not necessary in this kind of procedure. The most common suture materials used in equine laparoscopy include absorbable suture such as polyglactin 910 (Vicryl), lactomer (Polysorb), and polydioxanone suture (PDS II). The main problem encountered in horses is the length of the suture when the surgeon wants to use the extracorporeal knot-tying technique. The 135-cm length of # 3 or 150-cm length of # 2 polyglactin 910 sutures are particularly well suited for extracorporeal knot placement from the flank approach in the horse. Shorter sutures (90–120 cm) are adapted for intracorporeal knot-tying techniques.
The Simple Stitch
To make a simple stitch, the laparoscopic surgeon can choose between three options: making intracorporeal knots, making extracorporeal knots in the strict sense, or using an alternative as pushed half-hitches.
Introduction of the Needle and Suture into the Body and Loading of the Needle Holder
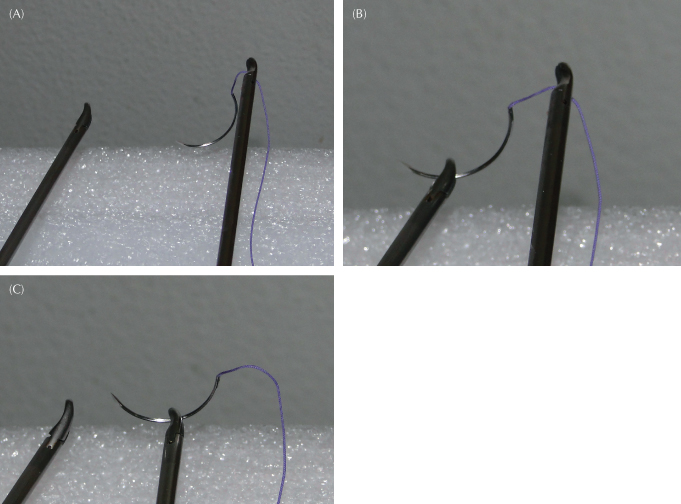
Under most circumstances, the needle and suture can be passed directly through the trocar. To pass the needle, the surgeon holds the suture with the needle holder 1–2 cm behind the swage of the needle. He or she will pay attention not to tear the gasket or valve with the needle. Once inside the peritoneum, the needle should be visible at all times for safety. To grasp the needle perpendicularly, the tip of the needle is grasped by a holding forceps. Then, by combining a rotation of this forceps and traction and repulsion of the thread using the needle holder, the needle can be placed in a perfect position, usually 90°, against the fixed jaw of the needle holder and grasped (Figure 3.6A–C, Video 3.3 at www.wiley.com/go/ragle).
Figure 3.6 Loading the needle in the needle holder in good position.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


