A ventrally positioned uterus can be returned to a normal, horizontal orientation by imbricating the two mesometria that suspend the uterine body and each horn (Brink et al. 2010) (Figure 19.2). By returning the uterus to its normal, horizontal position, uterine clearance may improve, which may restore fertility. Imbrication of the mesometrium to elevate the uterus has only recently been described (Brink et al. 2010), and insufficient numbers of mares have undergone the surgery to definitely determine the effectiveness of the procedure to improve fertility. The authors have used two different laparoscopic techniques to elevate the uterus.
Figure 19.2 A ventrally positioned uterus has been returned to a normal, horizontal orientation by imbricating the mesometria that suspend the uterine body and each horn.

Anesthesia, Positioning, and Surgical Preparation
The surgery is performed with the horse sedated and standing in stocks. Feed should be withheld for about 36 hours before surgery; otherwise, the large colon may obstruct the surgical site. Water, however, can be provided ad libitum. Administering an antibiotic pre- or postoperatively is optional. Feces are removed manually from the rectum, and a Foley catheter is inserted into the bladder to empty it and to keep it empty. The flank and the last three intercostal spaces of each side of the mare are prepared for aseptic surgery. Each of the three proposed sites of incision for laparoscopic portals in each flank is desensitized with 20 mL 2% mepivacaine HCl injected subcutaneously and intramuscularly.
The mare is sedated by administering a bolus of detomidine HCl (0.005–0.01 mg/kg, IV). For some difficult-to-restrain mares, administration of butorphanol tartrate (0.01–0.02 mg/kg, IV) may facilitate the procedure. Sedation can be maintained by administering detomidine by bolus, as needed, or by intravenously infusing detomidine (0.02 mg/kg/h) and butorphanol (0.01 mg/kg/h) at a constant rate.
Instrumentation
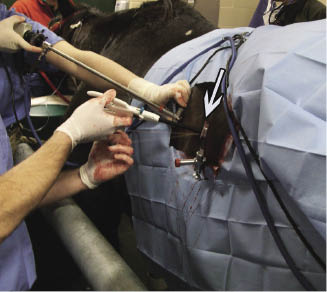
Laparoscopic instruments used to imbricate the mesometria vary depending on the method chosen. With either of the two methods, three trocar and cannula assemblies are used to visualize and access the mesometrium. For the cranial and caudal portals, we insert a 13.8-mm-diameter, 26.7-cm-long trocar and cannula assembly. At the middle portal, we insert a 25-mm-diameter, 31-cm-long trocar and cannula assembly. The barrel of a 60-mL syringe with the distal end of the barrel removed can be used as an instrument cannula, when positive pressure within the abdominal cavity is not needed (Figure 19.3). Using a shortened syringe barrel allows easier access to the uterine body if the instrument used for imbricating the mesometrium is too short to reach the uterine body when placed through a commercial cannula.
Figure 19.3 The barrel of a 60-mL syringe (arrow) with the distal end of the barrel removed can be used as an instrument cannula, when positive pressure within the abdominal cavity is not needed.
If the surgical site is easily visualized without using positive abdominal pressure, the valve of the portal used for suturing should be removed from the cannula before the trocar and cannula assembly is inserted into the abdomen. Removing the valve prevents suture inserted through the cannula from catching on the internal, one-way valve present in the cannula to maintain abdominal insufflation. An injection cannula with an 18- or 19-ga needle can be used to administer local anesthetic solution into the mesometrium to minimize painful reaction to the manipulation of the mesometrium and uterus.
Surgery
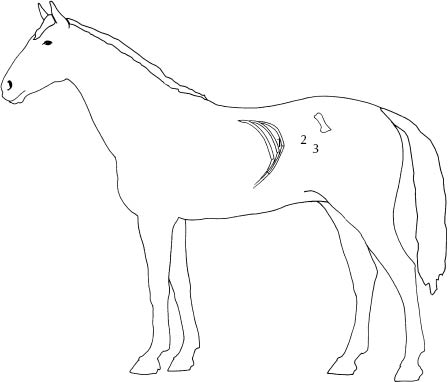
The left mesometrium is imbricated first so that the equilibration of intra-abdominal pressure with atmospheric pressure, which occurs when cannulas are placed through the left flank, causes the cecum to drop from the right paralumbar fossa, making inadvertent puncture of the cecum with a trocar and cannula less likely when portals are eventually placed in the right paralumbar fossa. Portal sites (Figure 19.4) for mesometrial imbrication are (1) the 17th intercostal space slightly below an imagined line drawn horizontally through the ventral border of the tuber coxae (i.e., the cranial portal), (2) a site midway between the ventral aspect of the tuber coxae and the last rib at the dorsal level of the crus of the internal abdominal oblique muscle (i.e., the middle portal), and (3) a site 6 cm ventral and 2 cm caudal to the central portal (i.e., the caudal portal).
Figure 19.4 Portal sites for mesometrial imbrication are (1) the 17th intercostal space slightly below an imagined line drawn horizontally through the ventral border of the tuber coxae, (2) a site midway between the ventral aspect of the tuber coxae and the last rib, and (3) a site 6 cm ventral and 2 cm caudal to the central portal.
The laparoscope is inserted into the abdominal cavity through the cannula at the cranial portal so that placement of the other cannulas can be observed. Using cannulas with a rubber valve at their exterior end so that positive pressure can be maintained within the abdominal cavity is often optional because positive pressure is usually not necessary to easily visualize and manipulate the uterine horns, provided that the mare has been properly fasted. If the uterine body is difficult to visualize because of interference of other viscera, the abdomen is insufflated with CO2 to a pressure of 10–12 mmHg. The cranial aspect of the uterine horn is often not visible because its abnormal, ventral orientation causes it to be obscured by other viscera, but the ovary can usually be readily identified.
Performing mesometrial imbrication on large breed, obese mares can be difficult because the caudal portion of the uterine body is often difficult to reach with the instruments. Restricting the diet of a large, obese mare for 1–2 months before attempting mesometrial imbrication may be beneficial in improving access to the surgical site and maneuverability of instruments.
The mesometrium is imbricated using a laparoscopic needle holder or an endoscopic automated suturing device. To imbricate the mesometrium using an endoscopic needle holder, the uterine body and the left uterine horn are sutured to the mesometrium with a 1.5-m strand of 8-metric (6) polyglactin 9102 swaged to a large, round-bodied, trocar-point, half-circle needle.
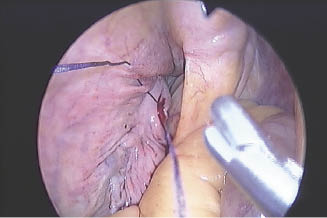
The suture and needle holder are inserted into the abdomen through the large (25-mm diameter), middle cannula. Using a laparoscopic Babcock forceps or another needle holder inserted through the smaller caudal cannula to stabilize the uterus, the needle is inserted through seromuscular layers of the dorsolateral aspect of the body of the uterus, adjacent to the reflection of the mesometrium onto the uterus, and then through the mesometrium about 3 cm dorsal to its attachment on the uterus (Figure 19.5).
Figure 19.5 To place the first suture, the needle is inserted through seromuscular layers of the dorsolateral aspect of the body of the uterus, adjacent to the reflection of the mesometrium onto the uterus, and then through the mesometrium about 3 cm dorsal to its attachment on the uterus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


