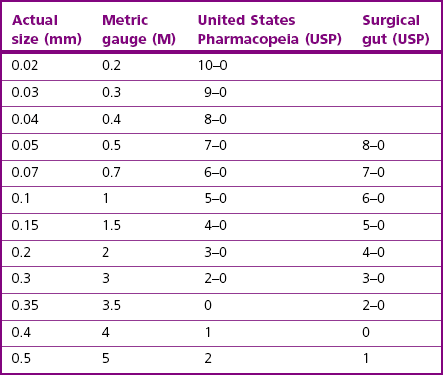
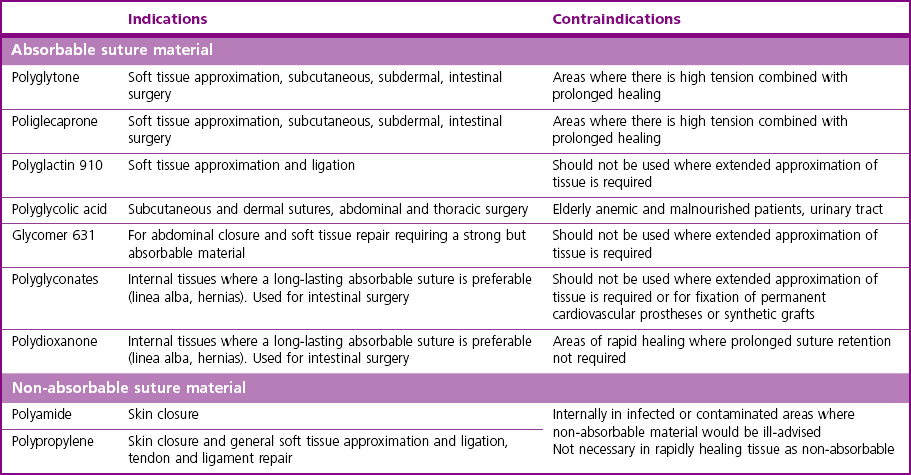
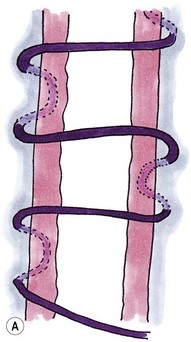
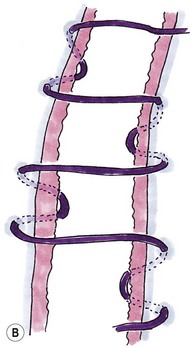
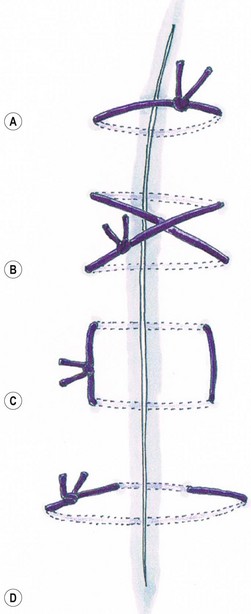
Chapter 10 The smallest diameter suture material that will adequately hold the healing tissue should be used. In cats, size 1.5–3 metric gauge (M) will be suitable for most general use. For either very delicate work or areas where a higher tensile strength is required, sutures outside this size range may be needed. Size conversion for suture materials is shown in Table 10-1. Natural materials like silk, cotton, ovine intestinal submucosa, or bovine serosa (catgut) can cause inflammatory reactions within the tissues and their absorption, by phagocytosis, may be variable depending on implant site and patient status. Synthetic materials are usually chemical polymers absorbed by hydrolysis, and thus they often have a more predictable rate of absorption independent of these factors (Table 10-2). Table 10-2 Loss of strength and absorption times of suture materials Modifications to several of the generic suture materials include the introduction of rapidly absorbable sutures (the ‘Rapide’ range) and sutures with improved resistance to bacterial penetration (the ‘Plus’ range). The ‘Plus’ range sutures, which include polyglactin 910, polydioxanone and poliglecaprone, are coated with triclosan, which is an inhibitor of bacterial fatty acid synthesis with demonstrable antibacterial activity. The use of triclosan-coated sutures in humans has been associated with a decreased infection rate.1 Careful attention to proper suturing technique and use of the appropriate suture patterns for wound closure is important in ensuring optimal closure and incisional healing. Careless handling of the suture or the use of damaged instruments can weaken the suture and make it more prone to breakage. Eversion of skin edges or excessively tight skin sutures can encourage self-trauma by the patient, increasing the risk of suture line infection or premature suture removal by the cat. Excess tension on sutures in wound closure can lead to ‘cutting out’ of sutures or to ischemia of tissue adjacent to the sutures. In areas of tension, the surgeon should consider other techniques such as the use of subcutaneous walking sutures, undermining of the skin, tension-relieving sutures, and then surgical procedures, including relaxing incisions, plasty procedures, or skin flaps (see Chapter 19). Suture patterns commonly used in feline general surgery are shown in Figures 10-1 and 10-2. There are several different suture materials on the market (Table 10-3) with a variety of different properties, indications and contraindications. The materials available in practice will vary according to surgeon preference and procedures commonly performed. The indications and contraindications for the different suture materials are listed in Tables 10-4 and 10-5. Table 10-3 Suture materials and some commercial manufacturers Table 10-5 Suture recommendation for various tissue types Figure 10-1 Simple sutures: (A) simple interrupted; (B) cruciate mattress; (C) vertical mattress; and (D) horizontal mattress. Catgut is made of collagen obtained from bovine intestines. It is naturally degraded by the body’s own proteolytic enzymes. It can cause a significant foreign body reaction when implanted in tissues. Absorption is unpredictable, occurring faster in patients with cancer, anemia, and malnutrition or when used in gastric surgery, an infected wound, or highly vascularized tissue.2 It is also absorbed faster when used in the mouth and in other mucous membranes, e.g., vagina, due to the presence of microorganisms. In one study of 12 cats where suture material was implanted into the oral cavity it completely disappeared between days 3 and 7.3 It was used in a prospective study for all ligatures and closure of the linea alba in routine ovariohysterectomies in 24 cats.4 Dehiscence did not occur in any of the cats; however, the author has seen dehiscence of the linea alba after celiotomy closure and would recommend alternative suture material such as polydioxanone or glycomer 631 be used in this situation. Poliglecaprone is commonly used for subcutaneous and subdermal tissue closure. Careful technique ensuring an adequate number of throws, good knot security and sufficient purchase of tissue with each bite should be taken when placing in areas of high tension. It causes a relatively short-lived inflammatory response. Polyglycolic acid (PGA) suture is classified as a synthetic, absorbable, braided multifilament. It is coated with N-laurin and l-lysine, which render the thread extremely smooth, soft, and safe for knotting. It is also coated with magnesium stearate and finally sterilized with ethylene oxide gas. It is naturally degraded in the body by hydrolysis and has approximately 60% strength left at 14 days; absorption is completed between 60 and 90 days. It has the advantages of high initial tensile strength, smooth passage through tissue, easy handling, excellent knotting ability, and secure knot tying (better when wet). It is commonly used for subcutaneous sutures, intradermal closure, abdominal and thoracic surgeries. Elderly, anemic and malnourished patients may absorb the suture more quickly. Absorption is faster in urine, and so it is not recommended for urinary tract surgery.5 Polydioxanone was still intact at day 28 in the oral cavity of cats, and it is recommended for procedures in which longer healing time is anticipated3 such as hernia repair or pexy procedures.
Sutures and general surgical implants
Suture materials
Selection of suture materials
Suture material composition
Loss of strength in weeks (percentage loss)
Absorption time in days
Intestinal submucosa (catgut)
2–3 (100%)
14–80 approx
Polyglytone
2–3 (100%)
56
Poliglecaprone
1–2 (50%)
119
Polyglactin 910
2–3 (50%)
56–70
Polyglycolic acid
2–3 (50%)
90
Glycomer 631
2–3 (50%)
90–110
Lactomer
2 (20%)
56–70
Polydioxanone
4–6 (50%)
180
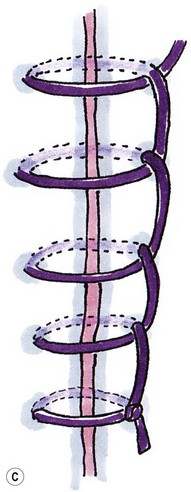
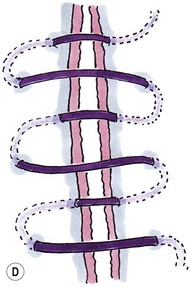
Suture placement and patterns
Suture material
Manufacturer
Catgut
Polyglactin 910
Vicryl: Ethicon, Polysorb: USS/DG
Poliglecaprone
Monocryl: Ethicon
Polyglycolic acid
Dexon II: USS/DG, Safil: Braun
Polyglycomers
Maxon: USS/DG, Monosyn: Braun
Polydioxanone
PDS: Ethicon
Glycomer 631
Biosyn: USS/DG
Polyglytone 6211
Caprosyn: USS/DG
Nylon, polyamide
Monosof: Covidien, Ethilon, Nurolon: Ethicon, Dafilon: Braun, Supramid: Braun, Dermalon: USS/DG, Monosof: USS: DG, Surgilon: USS/DG
Caprolactum
Vetafil
Polypropylene
Prolene: Ethicon, SurgiproII: USS/DG, Premilene: Braun
Polyester
Surgidac: USS/DG, Ti.Cron: USS/DG, Mersilene: Ethicon, Ethibond Excel: Ethicon, Miralene: Braun, Dagrofil: Braun, Synthofil: Braun, PremiCron: Braun
Polybutester
Novafil: USS/DG, Vascufil: USS/DG
Silk
Perma-hand: Ethicon, Sofsilk: USS/DG, Silkam: Braun
Stainless steel
Steel: USS/DG, Flexon: USS/DG, Surgical Stainless Steel Suture: Ethicon, Steelex: Braun
Tissue types
Suture recommendation and contraindications
Skin
Monofilament non-absorbable, e.g., polyamide or polypropylene
Subcutaneous
Absorbable, e.g., poliglecaprone, polyglactin 910, polyglytone
Tendon
Strong non-absorbable or slowly absorbable, e.g., polydioxanone, polypropylene, polyamide
Abdominal closure – linea alba
Strong, with good knot security (use extra throws), e.g., polydioxanone, glycomer 631
Muscle
Absorbable, e.g., polyglactin 910, polyglycolic acid, glycomer 631
Parenchymal organs
Absorbable monofilament, e.g., poliglecaprone, glycomer 631
Hollow viscus
Absorbable, e.g., poliglecaprone, polyglactin 910, glycomer 631
Avoid polyglycolic acid in the bladder as it rapidly dissolves in urine
Infected or contaminated wounds
Absorbable g. polyglactin, poliglecaprone.
Avoid braided non-absorbable sutures which can fistulate or catgut which rapidly absorbs
Vessels and vascular anastomoses
Ligatures – absorbable suture material
Vascular anastomoses – non-absorbable monofilament, e.g., polypropylene and with a needle-to-suture ratio of 1 : 1
Absorbable suture materials
Catgut
Poliglecaprone 25
Polyglycolic acid
Polydioxanone
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Veterian Key
Fastest Veterinary Medicine Insight Engine