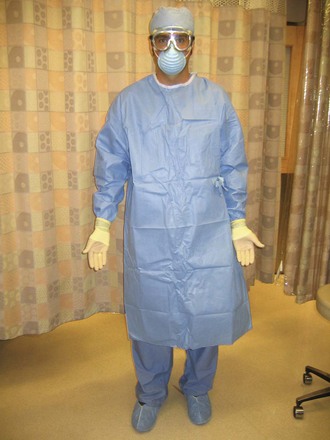
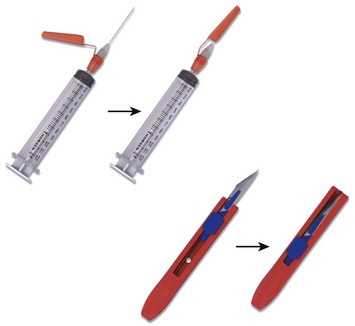
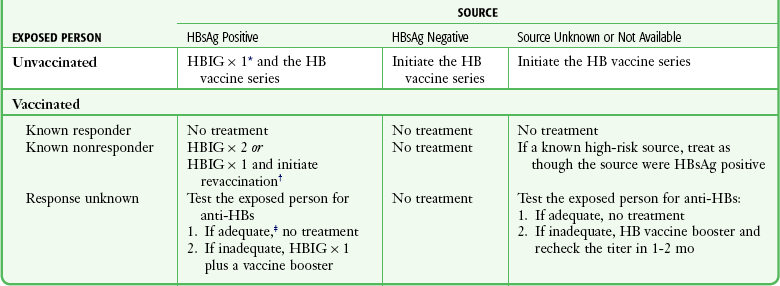
Chapter 68 Contamination of health care workers with body fluids is a frequent occurrence in the emergency department (ED). A survey of ED staff found that 54% reported contact of intact skin with body fluids and 1.5% reported contact of nonintact skin within the preceding year.1 These fluids often contain various transmissible infectious diseases because the prevalence of human immunodeficiency virus (HIV) infection, hepatitis, and other communicable diseases is high in ED patient populations.1,2 In a prospective study of penetrating trauma patients admitted to an urban trauma center, 9% tested positive for anti-HIV, hepatitis B surface antigen (HBsAg), or anti–hepatitis C virus (HCV). Patients were infrequently aware of their seropositive status.2 In the ED, patient characteristics were found to be poor predictors of hepatitis positivity, thus making it more difficult to identify patients who pose a risk to health care workers.3 These factors make widespread use of universal precautions in the ED essential. Compliance with standard precautions, formerly known as universal precautions, is far from universal.4–6 In a video-taped observational study of 88 ED trauma resuscitations, 33.4% had major breaks in standard precautions. The most common major break was failure to wear a mask (32.2% of procedures), followed by inadequate eyewear (22.2%), no gown (5.6%), and no gloves (3.0%).6 Henry and colleagues showed that ED personnel significantly overestimate their use of standard precautions.7 In 1985, the combination of high-risk illness with low-compliance barrier use prompted the Centers for Disease Control and Prevention (CDC) to recommend guidelines for the protection of health care workers.8 In 1991, these recommendations were enacted into law by mandate of the Occupational Safety and Health Administration (OSHA).9 The primary focus of the CDC guidelines is to reduce mucocutaneous exposure to body fluids by encouraging hand washing and barrier protection. These measures do little to protect from percutaneous exposure, which is the most efficient method of transmission of hepatitis and HIV.10,11 The current strategy for risk reduction in the ED includes immunization against hepatitis B virus (HBV), use of standard precautions (including reengineered safety products), and prompt initiation of postexposure prophylaxis (PEP) when appropriate. 1. Use gloves for any patient contact with a risk for exposure to body fluids (Fig. 68-1). Both cutaneous and percutaneous exposure can be reduced by the use of gloves. Gloves have been shown to reduce disease transmission in needlestick injuries, with greater reduction seen with double gloving in animal models and in a case crossover study of health care workers.12 Mansouri and associates compared the biomechanical performance of single and double latex and nitrile examination gloves. Transmission of red blood cells was less with nitrile gloves than with a single layer of latex gloves despite being thinner than the latex examination gloves. A double layer of latex gloves provided the best protection in this study.13 2. Wear a mask and protective eyewear when exposure to body fluid aerosols is possible (e.g., wound irrigation, traumatic chest wound) (Fig. 68-2). 3. Wear a gown and shoe covers when there is the risk for large volumes of splashed body fluids (e.g., chest tube, thoracotomy) (Fig. 68-3). Most importantly, sharps precautions mean no recapping, bending, or breaking of needles. If needle recapping is deemed necessary, use a single-handed technique (Fig. 68-4). A safer alternative is to immediately dispose of the needle in an approved sharps container without recapping. In an observational study of ED employees, the rate of needle recapping was 34%, with most practitioners using a two-handed technique.14 Various reengineered products are available for use in the ED, including retracting scalpels, auto-capping needles, and needleless intravenous systems (Fig. 68-5). Using such devices decreases percutaneous injury rates among health care workers.15,16 A survey of infection control professionals at Iowa and Virginia hospitals found that implementation of such devices was the most common action taken to decrease percutaneous injuries.17 U.S. federal law now requires the use of safety-engineered sharps devices to protect health care workers. In brief, the Needle-stick Safety and Prevention Act of 2000 required the use of safety-engineered sharps devices to protect health care workers from needlestick injuries.18 A review of data from the Exposure Prevention Information Network (EPINet) sharps injury surveillance program estimated that needlestick injuries have decreased by 34% overall, with a 51% decline in nurses since the implementation of federal legislation.16 During contact with patients who have suspected or confirmed pulmonary tuberculosis (TB), wear a National Institute for Occupational Safety and Health (NIOSH)–approved N-95 particulate respirator (Fig. 68-6). These masks are designed to efficiently filter 1- to 5-µm particles and are less costly and more comfortable than high-efficiency particulate air (HEPA)–filtered masks. In addition, place such patients in a respiratory isolation room with negative pressure, high circulation (optimally at least 12 air changes per hour), and external exhaust. While in the ED, avoid procedures resulting in increased release of infectious droplets, such as sputum induction. Make sure that all potentially infectious patients wear a surgical-type mask, especially during transportation outside the respiratory isolation room (e.g., to radiology).19 Implementation of the CDC guidelines is variable. A study of three California hospitals in which CDC guidelines and hospital procedure were compared with actual practice found that 19% of patients with TB were not in negative pressure rooms. Of the 62 health care workers observed using a respirator for TB, 65% did not use it properly.20 Immediately wash any skin surface coming in contact with body fluids with soap and water. If performed properly, both soap and water and alcohol-based products are generally efficacious in removing bacteria.21 Soap and water perform better in removing Clostridium difficile spores,22 but alcohol-based products are preferred and may be more viricidal.21,23 In most health care settings, hand-washing rates remain low.24–26 HBV is a well-recognized occupational risk for health care providers, and multiple studies have documented the high prevalence of hepatitis in ED patients.3,27–29 An estimated 100 to 200 health care workers have died annually during the past decade because of the chronic consequences of HBV infection.30 Despite the attention focused on transmission of HIV, the infectivity of HBV is significantly higher. HBV is a more virulent organism and requires a relatively small inoculum for transmission.31 Percutaneous injuries are the most efficient mode of HBV transmission, but many infected health care workers do not recall a specific injury.32 Many body fluids other than blood contain HBsAg, but levels of infectious HBV particles in blood-free body fluids are 100 to 1000 times lower than in blood itself. Although human saliva alone does not appear to pose a significant risk for transmission of disease, human bites have been associated with transmission of HBV.33 Implementation of the CDC’s standard precautions, along with the OSHA regulations for barrier protection and preexposure vaccination, has led to a decrease in the incidence of HBV transmission.34 To understand the risk of HBV transmission resulting from occupational exposure, an understanding of a few key serologic markers for HBV is essential. HBsAg is a marker of active infection in the source patient. From a practical standpoint, HBV can be transmitted when HBsAg is present, and it is not generally transmissible when this marker is absent. Hepatitis B surface antibody (HBsAb) is a protective antibody against HBV. In vaccinating health care workers, the goal is to stimulate the immune system to produce a sufficient quantity of this antibody. Hepatitis B e antigen (HBeAg) can be found in the bloodstream of HBV-infected individuals during times of peak virus replication. When a source patient is positive for HBeAg, the bloodstream contains a much larger number of infectious HBV particles. If a nonimmune individual sustains a needlestick from an HBsAg-positive patient, the risk for HBV transmission depends on the HBeAg status of the source. The risk for clinical hepatitis is approximately 2% (range, 1% to 6%) if HBeAg is absent as opposed to a risk of 22% to 31% if HBeAg is present.35 PEP following exposure to an HBsAg-positive source may require hepatitis B vaccine, hepatitis B immunoglobulin (HBIG), both, or neither (Table 68-1). This depends on the vaccination and antibody response status of the exposed health care worker. HBIG is derived from pooled human plasma and provides passive immunization for nonimmune exposed individuals. This preparation is very safe and not known to transmit disease.34,35 When HBIG is used for PEP, give it ideally within 24 hours after exposure, and note that it is of questionable value beyond 7 days.36 PEP for HBV is remarkably effective, and infection is unlikely to develop in individuals who receive PEP.30 Hepatitis B vaccine may also be given with PEP. Individuals who have not previously been vaccinated or who have not demonstrated an adequate response should receive the hepatitis B vaccine. Adverse reactions to the hepatitis B vaccine are generally quite mild, and it is safe to give during pregnancy. For primary immunization, give an initial intramuscular injection, followed by subsequent intramuscular vaccinations at 1 and 6 months. Check antibody levels (HBsAb) at 4 to 6 weeks after the series is completed to confirm that the desired titer of at least 10 mIU/mL has been attained. Vaccinated individuals who achieve this antibody level are referred to as “responders” and are believed to be immune for life. Although 25% to 50% of vaccine responders demonstrate a decline in HBsAb levels to below 10 mIU/mL within 5 to 7 years, these individuals are still protected against clinical disease because of a robust immune system memory or anamnestic response.37 There is no need to provide vaccination or to check titers in individuals who have previously had an adequate titer.30 PEP with these agents is not contraindicated during pregnancy or lactation. Health care workers who have previously been infected with HBV are immune to reinfection, so PEP is not indicated in such individuals. TABLE 68-1 Recommendations for Hepatitis B Prophylaxis after Percutaneous or Permucosal Exposure HB, hepatitis B; HBIG, hepatitis B immunoglobulin; HBsAg, hepatitis B surface antigen. *HBIG dose = 0.06 mL/kg intramuscularly. †The option of giving one dose of HBIG and reinitiating the vaccine series is preferred for nonresponders who have not completed a second three-dose vaccine series. For persons who previously completed a second vaccine series but failed to respond, two doses of HBIG are preferred. ‡Adequate anti-HBs = 10 mIU/mL. Adapted from Panlillio AL, Cardo DM, Grohskopf LA, et al. Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV and recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2005;54(RR-9):1-17. Approximately 1.6% of Americans (4.1 million) are infected with HCV,38 and many individuals are unaware of their infection. ED patients have a higher prevalence than the general population. In one study the prevalence of HCV antibody was 4.0% as compared with a prevalence in the overall U.S. population of 1.8%.27 HCV is often acquired from injection drug use. It was once commonly transmitted by blood transfusion but is fortunately rare now with modern screening. Although HCV can be transmitted sexually, this a minor route. Mucous membrane transmission of HCV is possible but much less common. Percutaneous transmission is the most efficient route. The incidence of seroconversion after an HCV-positive needlestick is about 1.8% (estimates range from 0% to 7%).35 It is useful to remember that the risk for transmission of HCV after a needlestick is similar to that for transmission of HBV when the source is HBeAg negative. When seroconversion does occur, 80% of patients will demonstrate antibodies at 15 weeks and 97% at 6 months after exposure. Although the clinical course of HCV is often asymptomatic or mild, chronic hepatitis will develop in approximately 85% of patients, cirrhosis in 10% to 20%, and hepatocellular carcinoma in 1% to 5%.39–41 According to the CDC, 57 cases of occupational HIV transmission to health care workers occurred in the United States through 2010. In addition, another 143 health care workers demonstrated HIV seroconversion that may have been occupationally related.43 The risk for contracting HIV from working in the ED depends on the prevalence of HIV in the local patient population. Wears and coworkers44 estimated the cumulative career risk of contracting HIV from occupational exposure in a high-prevalence ED to be as high as 1.4%. The overall risk for HIV seroconversion is about 1 in 300 (0.3%) after a needlestick and less than 1 in 1000 for mucous membrane exposure. Cardo and colleagues45 demonstrated that the risk for HIV seroconversion after needlestick injuries is not uniform. Seroconversion was found to be more likely for deep injuries (odds ratio [OR] = 15), if blood was visible on the device (OR = 6.2), if the needle had been used in a source patient’s artery or vein (OR = 4.3), or if the source patient suffered from terminal acquired immunodeficiency syndrome (AIDS; OR = 5.6). It is essential to gather information regarding the nature of the injury to “risk-stratify” the exposure. Exposure of intact skin to contaminated blood has not been identified as a risk for transmission of HIV.46,47 When seroconversion occurs, HIV antibodies can be detected as early as 3 weeks after exposure and are almost always present by 6 months. Seroconversion at 6 to 12 months is rare but has been reported in individuals co-infected with HIV and HCV. Follow-up HIV testing is recommended for 12 months for health care workers who become infected with HCV after dual exposure to both HCV and HIV.46 Acute retroviral syndrome is a clinical manifestation of HIV seroconversion that occurs in approximately 80% of newly infected individuals at a median of 25 days after exposure. The signs and symptoms of acute retroviral syndrome are similar to those of mononucleosis and consist of fever, lymphadenopathy, and rash.
Standard Precautions and Infectious Exposure Management
Guidelines for Standard Precautions
Barrier Precautions
Sharps Precautions
Respiratory Precautions
Hand Washing
Occupational Disease Exposure
HBV
Postexposure Management
HCV
HIV
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Standard Precautions and Infectious Exposure Management