Chapter 37 Squamous Cell Carcinoma in Buceros Hornbills
The rhinothecal ornamentation known as the casque is unique to the avian family Bucerotidae (hornbill).9 The casque is an air-filled cavity with minimal cancellous bone caudally in all but one species, the greater helmeted hornbill (Buceros [Rhinoplax] vigil).7 This space is enclosed by a thin shell of bone and overlaid externally by keratin. The striking external casque contours and rhamphothecal coloration varies by species, gender, and sexual maturity.
Casque squamous cell carcinoma (CSCC) has been documented repeatedly in great hornbills (Buceros bicornis), also called concave-casqued, great pied, giant, or great Indian hornbills, since the incident case was described in the literature in 1985.7,9,12 Despite two other species in the genus and one species (Buceros [Rhinoplax] vigil) in a closely related genus, it is only the great hornbill that has presented this specific pathology. No such casque neoplasia has been presented in any other of the 50 extant hornbill species, although 27 others are found in Asia, and are even sympatric with Buceros in India, Thailand, Java, Sumatra, Vietnam, and southwestern China.
Great hornbills were exhibited in Association of Zoos and Aquariums (AZA) holding institutions without successful captive breeding until 1973.13 Largely through importation, the managed population of great hornbills in the United States reached a maximum population of 79 in 1983. At the onset of active investigation of CSCC in 2006, only 52 birds were present in this group and, currently, the Species Survival Plan (SSP) reports only 43 individuals in 18 institutions. The great hornbill is slow to mature, requiring 5 to 6 years to reach phenotypic maturity, and unlikely to reproduce successfully before 10 years.9 It is also long-lived, with more than 40 years not unexpected, although its median longevity is 10 to 13 years. The species has not been reported to breed successfully beyond 30 years of age, when CSCC typically presents; however, six animals in the affected group were actively courting, mating, or nesting at the time of their diagnosis. Considering that the U.S.-managed population generally hovered between 40 and 50 individuals in the last 25 years, and that not all of these animals were adults, removal of 11 adults represents a loss of 20% of the population, which has not been counteracted by slow captive reproductive success.
Squamous cell carcinoma has been diagnosed previously in other avian species. It has been documented at the cere or in the oral cavity, but has not been reported previously with such a species-specific predilection.12,14,15 Through 2010, 12 cases of CSCC in great hornbills have presented similarly in onset and progression, and consistently in location on the casque and rhinotheca. Until recently, only birds in AZA-holding institutions were reported, despite repeated inquiries to European Endangered Species Program–holding institutions.8 However, in 2008, a single case was reported in the United Kingdom.1
Clinical Presentation
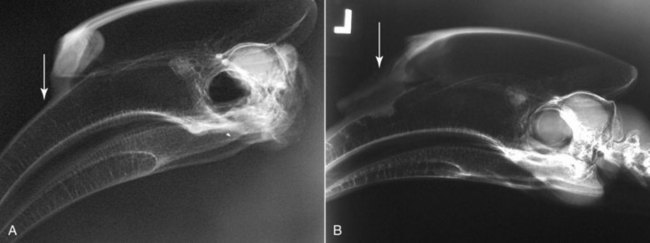
The hornbill casque has a location vulnerable to trauma and environmental damage because of its protrusion from the rhinothecal contour. In the great hornbill, the square-ended rectangular casque interfaces with the maxillary beak rostral to the external nares by approximately 50% of the casque length (see Fig. 37-2,A).7 It is at this interface—the rostroventral casque and dorsocaudal maxillary rhampotheca—that CSCC consistently appears. In five of the CSCC-group, diagnoses of trauma, frostbite, bacterial sinusitis, or fungal infection of the casque were made prior to conclusive determination of neoplasia.
The external clinical presentation of CSCC is often limited to a focal softening, fissuring, or discoloration of the rostral casque or, occasionally, the maxillary rhinotheca near the casque, rather than the ulceration typically reported in other avian species.14 Black, grey, or brown dry flaking tissue or actual necrosis with pink fleshy material is often found in the rostral casque once the bird is manually restrained and the abnormal keratin is debulked (Fig. 37-1). In warmer climates or seasons, myiasis has presented as a confounding problem. In several cases, before lesion identification, a pervasive yeast or necrotic odor was noted in the animal’s enclosure or associated with the animal specifically. Although most of the birds had uneventful clinical histories prior to CSCC, three of them had notations of lost pieces of casque 1 to 4 years prior to CSCC diagnosis, and one had a notation of lost casque pieces and partial casque slough 11 years preceding neoplastic presentation.

Diagnosis
The full extent of CSCC is better appreciated by imaging. Simple radiography may detect soft tissue opacification of the affected areas, sinuses of the casque or maxillary beak, and potential bony invasion (see Fig. 37-2).7 Multiple radiographic views may assist in staging debulking of the neoplasm but lateral images of the skull and casque will screen most rapidly for the presence of the neoplasm. These particular images are easily obtained under manual restraint, with the head and neck secured by tape or while the bird is fully anesthetized. Although advanced imaging has been performed in Buceros species, it is not considered necessary for conclusive CSCC diagnosis.18
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


