Chapter 32 Small Mammal Dentistry
Equipment
The dental equipment required for pet rabbits and other small mammal species falls into two groups: instruments for diagnosis and instruments for treatment.13,14
Because of the small, long, narrow oral cavity of rabbits and herbivorous rodent species, mouth gags are essential instruments for oral examination under general anesthesia. Special mouth gags designed for rabbits and rodents fit with the clinical crowns of incisors, but these gags should be used with extreme care to prevent excessive stretching of the masticatory muscles and the ligaments of the temporomandibular joint. Be aware that wide opening of the oral cavity is not a natural movement for herbivorous elodont species. The “rabbit and rodent table retractor/restrainer” (also named: “tabletop mouth gag”) is a special platform acting as a combined mouth gag and patient positioner. The second essential instrument to access the oral cavity of rabbits and rodent species is the cheek dilator. Different sizes and shapes are available. Longer blades fit better into the rabbit mouth and are more effective in dilating cheeks. A small, modified “open blade” (rather than flat) cheek dilator is especially designed for rodents, but it also works well for dwarf rabbits weighing less than 1 kg. It is particularly useful in guinea pigs because of the double-folded cheek opening in this species.
Special instruments for intraoral dental treatment are needed. Elevators for rabbit incisor and cheek teeth have been specially designed.32 Small extraction forceps can be used to extract incisors; needle holders and small hemostats can be used as well, depending on the patient’s size. For rodents, appropriately contoured needles are used for extracting incisors and are shaped to match the size and curvature of the tooth. A dental unit is recommended for dental treatment of small mammal species. While not necessary for ferrets and other carnivorous or omnivorous species, a straight dental handpiece is needed for intraoral treatment of rabbits and herbivorous rodent species. Many different types, shapes, and sizes of burrs are available. Diamond rasps and cutters for rabbit cheek teeth are available, but their use must be discouraged because forces applied by these instruments can cause fractures of cheek teeth and severe damage to adjacent soft tissues.
Diagnostic Testing
The Clinical Examination
Dental disease is a syndrome and can produce a wide range of clinical signs and symptoms.13 These may be related specifically to the primary dental problem (reduced food intake, anorexia, dysorexia, dysphagia, changes in fecal quantity and size, weight loss) or to complications associated with dental disease (excessive grooming, excessive salivation and drooling, facial abscesses, epiphora, exophthalmos, nasal discharge, dyspnea). Other signs and symptoms are indicative of diseases or conditions secondary to dental disease (poor general condition, gastrointestinal problems, poor coat and skin diseases, ocular diseases, death).13,58
Before performing a physical examination, obtain a thorough history and review the diet and feeding habits with the owner. Considering the capability of prey species to mask or hide symptoms, the absence of a clear clinical history does not rule out the possibility of dental disease. Reduced food intake and abnormal feces in rabbits and rodents are common early symptoms frequently missed by owners. A thick hair coat can hide evident signs like weight loss or the presence of facial swellings. Use careful and proper restraint during a dental examination.13,32
In unsedated rabbits and some large rodents, the oral cavity can be inspected with an otoscope. A plastic otoscope cone is preferable to a metal instrument because the latter might cause iatrogenic dental fracture if the animal chews on it. However, if used carefully, a nasal speculum with an attached light source is helpful in viewing spurs, elongated crowns, or buccal or lingual ulcerations. Include examination of the eye and periocular structures in the dental examination. Evaluate patency of the nasolacrimal duct in rabbits by flushing with saline or with fluorescein dye (see Chapter 37). When dental disease is a presumptive or a differential diagnosis, complete the oral examination with the animal sedated or under general anesthesia.
Because of the natural behavior of most pet rodents, safe restraint and effective oral examination is much more difficult in unanesthetized rodents than in rabbits. Oral inspection other than that of the incisors is not feasible without sedation. Complete inspection and proper diagnosis of dental disease in rodent species must always be performed under general anesthesia.13
Imaging
Radiography
In rabbits with suspected dental disease, a full radiographic examination of the skull and teeth is an essential diagnostic tool.13,20 Deep sedation or general anesthesia is necessary for optimal positioning for radiographs. Although rabbits are routinely intubated for anesthetic procedures, the endotracheal tube may interfere with the radiographic image.13
Good-quality skull radiographs can be obtained with the use of standard or digital radiographic equipment (see Chapter 35). For standard radiography, ultra-slow-speed films, dedicated intensifying screens, and high-resolution mammography x-ray films are particularly advantageous.13,19
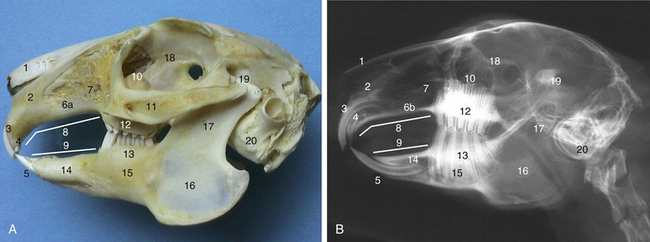
Multiple views are necessary to fully evaluate the dental anatomy. 13,20,70 Never base diagnosis and prognosis on any single radiographic image. In rabbits, include five standard projections in the radiographic series: lateral, left-to-right oblique, right-to-left oblique, ventrodorsal or dorsoventral, rostrocaudal.13,19,20,39 The lateral view is useful to evaluate the occlusion of the maxillary and mandibular incisors, the occlusal plane of the cheek teeth, and the overgrowth of clinical crowns (Fig. 32-1). The normal appearance of the occlusal plane of the cheek teeth is a zigzag line. An ideal oblique projection has minimal (15-20 degrees) rotation, and the contralateral oblique view should always be obtained for comparison. Each projection is especially useful to evaluate reserve crowns and apices of mandibular cheek teeth on one side of the head and the same dental structures of maxillary cheek teeth on the other. The ventrodorsal or dorsoventral view is useful to evaluate overgrowth of cheek teeth and deformities of the mandible. Superimposition of mandibular and maxillary structures impairs evaluation; shifting the tip of the mandible laterally permits visibility of an entire quadrant of maxillary cheek teeth. Ideal positioning in the rostrocaudal projection allows evaluation of the occlusal plane of the cheek teeth and the temporomandibular joints. Excellent symmetrical positioning is mandatory for both the ventrodorsal and the rostrocaudal projections.13,19,39 One or more intraoral dental views using small dental films may be useful in addition to the radiographic study of the skull and teeth. Either the standard radiographic equipment or a dental radiographic unit can be used.3,13,19,39
In rodents, either very high definition intensifying screens and films such as those used for mammography are critical for adequate detail.13 In guinea pigs, the normal bending of cheek teeth (see “Anatomy,” below) does not allow visualization of their occlusal plane on the lateral projection; the rostrocaudal projection is the only one allowing a proper evaluation.13,20,39
In ferrets, radiographs of the skull and teeth are very important when the oral examination suggests the possible presence of retained roots, periodontal infection or abscess, and osteomyelitis.21,55 Open-mouth projections and intraoral projections using small films can be added to standard projections.19 Mouth gags used in ferrets (Jorgensen Laboratories, Loveland, CO; www.jorvet.com) are miniature replicas of dog and cat mouth gags14 and are applied to the tip of canine teeth to open the mouth. When a radiotransparent device is needed for open-mouth radiographic projections, a presized piece of syringe can be used.
Oral Endoscopy
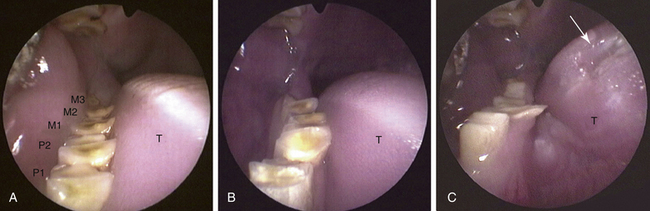
Even during examination of the anesthetized rabbit, experienced observers can still miss several lesions. Oral endoscopy allows thorough inspection of the oral cavity and greatly facilitates detection of subtle lesions because it provides magnified perspective of dental structures.10,13,48,49,74 Instruments for oral endoscopy are described in Chapter 34; normal and pathologic endoscopic patterns have been reported (see “Dental Disease,” below).8,10,13,49,60 While endoscopy is very useful in rabbits, it is an integral part of the examination in rodent species. Other magnification devices are helpful but not always sufficient, and many lesions can be missed without endoscopy.
Computed Tomography
Computed tomography (CT) has received great attention in exotic animal medicine during the past few years (see Chapter 35). With the advent of newer spiral CT scanners and the availability of postcapture image manipulation software, this diagnostic imaging modality has become feasible, practical, and extremely useful as an adjunct to standard radiography and provides excellent detail even in small mammals.5,16,19,20,22,28 CT is particularly useful over traditional radiography (visualization of the internal anatomy without superimposition of adjacent and overlying structures) in evaluating complications of dental disease such as facial abscesses and osteomyelitis.15,20,21,72 Optimal traditional radiographs (both digital and analog) still provide higher resolution, but CT allows visualization of important details impossible to see on radiographs because of the superimposition of different anatomic structures on a single plane. In selected cases, CT provides detailed diagnostic information that may be critical for proper prognosis and surgical planning of difficult dental cases.15,21 In particular, three-dimensional volume and surface renderings of the skull can provide excellent information for the diagnosis of dental disease or dental-related problems, such as abnormalities of the temporomandibular joint in guinea pigs.20
Other Diagnostic Testing
A complete blood count (CBC) and biochemical panel are routinely obtained in rabbits with dental disease.10 However, even in cases of periapical infection and abscessation, markedly abnormal findings in the CBC results are uncommon in rabbits.38 Unlike other species, where either leukocytosis and neutrophilia occur in response to bacterial infection, total leukocyte counts in rabbits rarely exceed two or three times the normal value.38,43 For these reasons, the CBC does not provide useful diagnostic or prognostic indications in cases of chronic bacterial infections and abscesses in rabbits. Laboratory findings are instead related to secondary diseases, when present, that may be associated with this syndrome.10
Bacterial culture and sensitivity testing is important in cases of periapical infections and abscesses.13,75,76 Anaerobic gram-negative and aerobic gram-positive pathogenic bacteria have been identified as causative agents, including Fusobacterium nucleatum, Prevotella species, Pseudomonas species, Streptococcus species, and Actinomyces israelii.1,75,76,81 Common rabbit pathogens such as Pasteurella multocida have not been isolated.76
Always request screening for both aerobic and anaerobic organisms when specimens are submitted for culture. Purulent material from the core of the abscess may be sterile and culture results of this are often unrewarding. A biopsy sample of the capsule wall obtained during surgical excision is more appropriate to submit for culture and sensitivity testing.13
Histopathology can be useful in selected cases, particularly when bone neoplasia is suspected.71
Rabbits
Anatomy and Physiology of the Skull and Teeth
Rabbits are highly specialized herbivorous placental mammals, and the evolutionary process has adapted the anatomy and physiology of the skull and teeth to accommodate their unique diet.13,26,33 Skull morphology is typical of true herbivores, similar to larger species like horses, cattle, sheep, and goats (see Fig. 32-1).13,32,64 The oral cavity is long and narrow, with a narrow opening. The temporomandibular joint is dorsal to the dental occlusal plane. Rabbits are anisognathic, with the mandible narrower than the maxilla.13,26,32,66 The incisors of lagomorphs are similar anatomically and partially functionally to those of rodents.13,26,32,33 For this reason, the order Lagomorpha was previously classified as a rodent suborder (Rodentia). However, lagomorphs differ from rodents because they have two pairs of maxillary incisors (duplicidentata), while rodents have only one pair (simplicidentata). Also, lagomorphs are diphyodont, with two sets of teeth (deciduous and permanent); while rodent species are monophyodont.13,25,26,33,43 However, this physiologic trait does not have practical relevance because the first set is shed before or immediately after birth. The labial maxillary incisors (also named: “first,” or “primary”), are bigger than the palatal incisors (also named: “second,” “secondary,” or “peg”). The mandibular and the maxillary first incisors are typically chisel-shaped. Rabbits lack canine teeth; incisors are separated from premolar and molar teeth by an edentulous gap (diastema). Premolar and molar teeth are anatomically similar and are therefore simply called “cheek teeth.” They are set closely together, without any significant interproximal space. As maxillary and mandibular cheek teeth differ in number, each mandibular tooth occludes with two maxillary cheek teeth, with the exception of the smaller first and sixth maxillary cheek teeth. The occlusal surface is not an even plane. Transverse ridges form a zigzag occlusal surface that can be seen as a zigzag line from a lateral view both on the skull and on a radiograph (see Fig. 32-1).13,26,32,33,43
All rabbit teeth are hypsodont (long-crowned), and elodont (continuously growing and erupting) teeth. They are defined as aradicular teeth because they do not develop anatomic roots. The anatomic parts of rabbit elodont teeth are the portion above the gingival margin (clinical crown), the portion below the gingival margin and inside the alveolous (reserve crown), and the open root (apex).13,26,33
The diastema separates the dental arcade into two functional units: the incisors and the cheek teeth. The function of the incisors of lagomorphs is to cut grass and other plants. Food is then chewed with the rough occlusal surface of the cheek teeth. Mandibular movements occur in three directions. Rostrocaudal movements are limited in lagomorphs.* Dorsoventral chewing movements similar to those of carnivores are very limited as well. Anisognathism explains the importance of laterolateral movements of the mandible. Because the mandibular dental arcades are closer to each other than the maxillary arcades, mandibular and maxillary cheek teeth are not in occlusion at rest. They come into occlusion alternatively, one arcade at a time, during chewing. Transverse ridges on the occlusal surface interlock with the opposite teeth during chewing, providing an efficient rough surface for grinding and crushing fiber.13,26,33,66
During normal chewing of fibrous foods, the clinical crowns of rabbit elodont teeth are constantly worn and continuously replaced by the reserve crown. The lateral movements allow wearing of the occlusal plane of primary incisors.13,26,43,66
Pathophysiology of Dental Disease
The pathophysiology of dental disease is mostly related to the continuous growth of teeth. Any process interfering with normal eruption or wear will result in some aspect of dental disease.13,32,33,66 Four different primary causes have been reported in the rabbit: congenital and developmental abnormalities, traumatic injuries, abnormal wear, and metabolic bone disease.† Congenital jaw mismatch may be caused by prognathism of the mandible or brachygnathism of the maxilla.13,32 This anatomic condition is common in purebred dwarf rabbits weighing less than 1 kg and in lop rabbits. Traumatic injuries often cause fracture of the incisors13; if the apex has been damaged, it may result in malocclusion. Fractures of the incisors that expose the pulp can lead to pulpitis and abscesses.
The most important and most frequent cause of dental disease is related to improper nutrition and abnormal wear.13,32,33 The natural diet of rabbits is rich in crude fiber and abrasive silicates. Even pet rabbits properly fed with hay and vegetables, including those kept in the garden eating the same kind of grass, do not receive the same types and variety of food as free-ranging lagomorphs. Therefore, all pet rabbits can potentially develop at least some subclinical degree of acquired dental disease during their lifetime.32,33 Moreover, despite the increased understanding of proper nutritional requirements, many pet rabbits are fed improper diets including seeds, bread, fruit, or treats and deficient in hay and vegetables. The pathophysiologic sequela follows a typical pattern, with few exceptions.13,32,33 The lack of fiber causes insufficient occlusal wear, and because teeth are elodont, the clinical crowns elongate. This elongation is partially counteracted by the strength of the masticatory muscles, and the increased pressure on cheek teeth (both at rest and during chewing movements) reduces elongation of the clinical crowns. This initiates two subsequent concurrent steps: bending of the axis of cheek teeth and elongating of the reserve crowns.
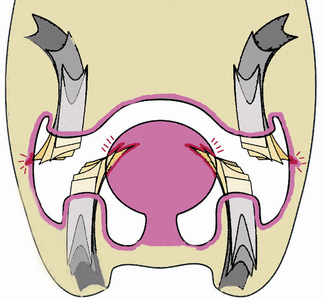
A cascade of abnormal changes then follows. Bending of the cheek teeth follows a typical pattern: the mandibular cheek teeth begin to bend medially (showing lateral convexity), while maxillary cheek teeth begin to bend laterally, with medial convexity. This further reduces the occlusal wear of cheek teeth arcades because the lateral chewing movements are not enough to fill the gap in occlusal surfaces. When occlusal planes begin to malocclude, the rabbit will reject hay, looking for food easier to crush (if available) and thus further reducing the amount of fiber and the lateral chewing movements. The occlusal planes do not wear on the lateral (buccal) margin of the maxillary cheek teeth and on the medial (lingual) margin of the mandibular cheek teeth, causing spikes and spurs to form (Fig. 32-2). These can be very sharp, creating discomfort and leading the rabbit to further reduce the degree of lateral chewing movement. Injuries and ulcerations of the tongue (from the mandibular cheek teeth) and the buccal mucosal surface (from the maxillary cheek teeth), often severe, represent secondary complications.
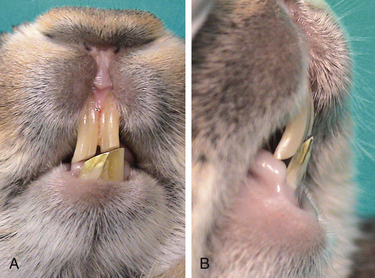
Excessively elongated cheek teeth, particularly the mandibular first premolars, may also lead to functional prognathism of the mandible.13,32 Once the crowns have elongated, the jaw is held more open and the mandible slides rostrally into a functional prognathic position, leading to malocclusion of incisors (Fig. 32-3). This condition is often incorrectly diagnosed as congenital, even in aging rabbits.
Metabolic bone disease as a cause of acquired dental disease has been extensively studied and reported.40,41,43,45 In a study in 81 pet rabbits, parathyroid hormone concentrations were abnormally high and calcium concentrations were low, suggesting metabolic bone disease as a predisposing condition for acquired dental disease.41 Most affected rabbits demonstrate demineralized skull bones and radiographic findings consistent with osteodystrophic disease of both the teeth and the skull bones. Demineralization of the bone matrix and weakness of the alveolar bone lead to loosening of the teeth, bending and rotation of the cheek teeth within the alveolus, and widened interproximal spaces. These changes lead to improper occlusion of cheek teeth and resulting abnormal wear of the clinical crowns. The ventral cortical bone becomes deformed, and the periosteum of the mandible and the maxilla eventually becomes perforated, leading to secondary complications such as abscesses.
Different pathophysiologic patterns (in particular abnormal wear and underlying metabolic bone disease) may be present in the same patient.
Dental Disease
The three most common clinical presentations of dental disease relate to overgrowth of the incisors, reduced food intake, anorexia or dysphagia, and presence of a facial swelling.13 Two or three of these conditions can be present at the same time. While dental disease affecting the cheek teeth is more frequent, diseases affecting the incisors are more apparent to the owners. Typically, the mandibular incisors tend to elongate labially, while the maxillary incisors tend to elongate palatally.13 For this reason, overgrown mandibular incisors usually do not produce secondary lesions because they are anterior to the upper lip and nose, while overgrown maxillary incisors curve dorsally and may damage the lips or the palate. Very elongated incisors may fracture. With end-stage dental disease, growth may be slowed or arrested. Dental disease of the incisors also affects the reserve crown. Abnormal elongation and apical deformity leads to partial or complete obstruction of the nasolacrimal duct. Epiphora, dacryocystitis, subsequent ocular lesions, or facial dermatitis are common possible sequelae (see Chapter 37).7,13,44,77
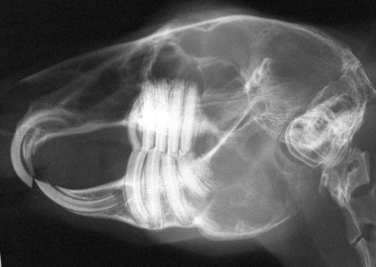
Rabbits with acquired dental disease of the cheek teeth may present at different stages. The earliest stage is elongated crowns. Radiographically the normal occlusal plane and its zigzag pattern are lost; the first premolars are curved, interproximal spaces widen, and the ventral profile of the mandibular cortical bone deforms slightly due to increased pressure (Fig. 32-4). Coronal elongation and the abnormal occlusal plane appear as “wave mouth” or “step mouth” on oral examination (Fig. 32-5).13,20 Clinical signs and symptoms are usually not present at this stage. In later stages, these abnormalities become more severe. Sharp spur and spikes may develop on the cheek teeth, leading to lesions of the tongue or the buccal mucosa (see Fig. 32-5). A common sequela of excessive coronal elongation of cheek teeth is fracture, especially longitudinal fracture of mandibular premolars.13 End-stage dental disease of the cheek teeth is frequently associated with resorption of bony and dental tissue.
The most common complications of acquired dental disease are periapical infections, osteomyelitis, and facial abscesses.13,18,43 The latter appear as large masses usually located at the ventrolateral aspect of the mandible or the lateral aspect of the maxilla. Some rabbits may show clear unilateral exophthalmos. Abscesses are typically firm, cool, and nonpainful. Early small masses are usually missed by the owners because of their location and the presence of fur, especially in long-haired rabbits.
Treatment of Dental Disease
In general, the goals of dental procedures are to reduce abnormal tooth length, to restore the occlusal plane to as near normal as possible, and to extract diseased teeth.59 Complications and secondary diseases like periapical infections, osteomyelitis, and abscesses are treated with combined dental procedures and extraoral surgery. Surgical treatment of diffuse osteomyelitis may require more invasive facial surgery.
Anesthesia of small mammals is discussed in Chapter 31. Many different anesthetic protocols are suitable for diagnosis and treatment of dental disease in rabbits and other small mammal species.57 Local anesthesia is an important adjunct for extraction of both incisor and cheek teeth.57,59
Medical Treatment
Medical therapy alone is generally inadequate for the treatment of dental disease but is an important adjunct to dental and surgical procedures. Medical therapy is aimed to address several concerns such as antibiotic, analgesic, and supportive treatment.13 In choosing an antibiotic, base the selection on both aerobic and anaerobic culture and sensitivity testing when possible, and consider any species-specific contraindications, such as oral administration of penicillins in rabbits and herbivorous rodents.13,43,68 Analgesia is critical to prevent pain-related anorexia. Supportive treatment includes hand-feeding products for convalescing small mammals, such as Oxbow Critical Care (Oxbow Pet Products, Murdock, NE, www.oxbowhay.com), especially for herbivorous species. Fluid therapy may also be necessary in some patients.13
Dental Procedures
Treatment of disease of the incisors includes coronal reduction and extraction.13,43,58 Coronal reduction is limited to cases in which the malocclusion is not severe and has been diagnosed early and proper occlusion of both incisor and cheek teeth can be restored. Reduction and reshaping of the incisors must be performed on anesthetized animals with low or high-speed dental equipment and appropriate burrs.23,32,33 Do not use trimmers, clippers, or similar instruments to cut overgrown or maloccluded incisors. These instruments do not allow the restoration of a normal incisal edge, and they frequently lead to complications such as fractures, damage of the apical germinative tissue, pulp exposure, endodontic infection, and periapical abscessation.12,13,30
The only definitive and completely effective treatment for severe malocclusion and acquired dental disease of incisors is extraction (Fig. 32-6).6,11,13,33 Rabbits adapt easily to lack of incisors, much better than when teeth are short or maloccluded, and they are able to eat normally using the lips and tongue to prehend food.
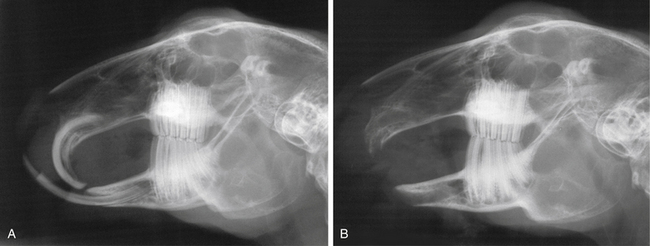
Fig. 32-6 A, Coronal elongation and malocclusion of the incisor teeth following congenital brachygnathism of the maxilla in a rabbit. The maxillary diastema is shorter than normal, and its length is similiar to that of the mandibular diastema (compare with Fig. 32-1, B). Cheek teeth are normal, including the zig-zag line at the occlusal plane. B, Postoperative radiograph after extraction of incisor teeth.
(Used by permission from Vittorio Capello, DVM.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


