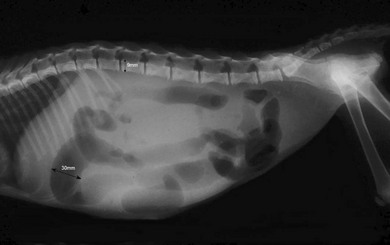
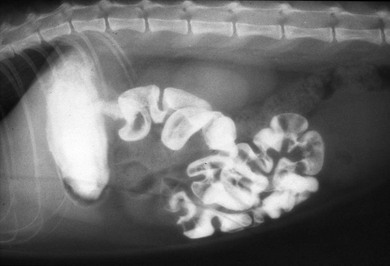
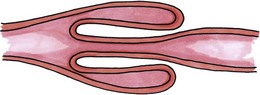
Chapter 29 The small intestine of the cat constitutes a simple continuation of the alimentary canal from the stomach to the large intestine, consisting of the duodenum, jejunum and ileum. The upper small intestine is primarily secretory and the lower small intestine primarily absorptive in function. Within the duodenum the location of the common bile duct and pancreatic ducts differs from the dog. The major duodenal papilla typically receives the common bile duct and major pancreatic duct, whereas a minor duodenal papilla is only present in cats, in which an accessory pancreatic duct persists. This reportedly occurs in approximately 20% of animals. Arterial supply to the small intestine is via branches of the cranial mesenteric artery and venous return is primarily by the cranial mesenteric vein, a major tributary of the hepatic portal vein. The intestinal wall consists of an outer serosa formed by visceral peritoneum, the tunica muscularis with its outer longitudinal, and inner circular layers. The submucosa, which is rich in collagen, also serves as the principal holding layer for sutures. The intestinal mucosa is lined by simple columns of epithelial cells mixed with variable population of mucus providing goblet cells. The cat’s microvascular anatomy is similar to that of dogs, with the vasa recta perforating the outer longitudinal and inner circular muscularis layers and supplying a rich submucosal vascular plexus. One distinguishing factor in cats is the presence of prominent lymphatic nodules in the mucosa, mostly along the antimesenteric aspect of the small intestine.1 In the cat (unlike the dog) it is as common to see anorexia and weight loss with intestinal obstruction as vomiting. It is essential to perform a thorough physical examination including abdominal palpation and oral examination. Cats are prone to ingestion of linear foreign bodies and sublingual examination will often lead to a quick diagnosis of yarn or fishing line entrapped at the glossal frenulum. One study of linear foreign bodies in cats reported a diagnosis rate of 75% using oral examination in combination with abdominal palpation (Fig. 29-1).2 In cats with intestinal disease, abdominal radiographs may reveal a radiopaque foreign body, loss of visceral detail, or an obstructive gas pattern. Small intestinal distension of greater than 12–14 mm is suggestive of intestinal obstruction in this species.3 Also, a quantitative index has been established in cats by calculating the ratio of the maximum small intestinal diameter/the dorsoventral cranial end plate measurement of the second lumbar vertebra. The probability of an intestinal obstructive is >70% if this ratio is greater than 3.0. (Fig. 29-2).4 Linear foreign bodies will often cause pleating of the jejunum, which can be noted on palpation. Likewise, pleating of the small intestine can sometimes be seen on plain films. If contrast material is used the clinician should avoid the use of barium sulfate and instead use an iodine-containing contrast in order to avoid the potential for granulomatous peritonitis (Fig. 29-3). Ultrasonography is also a sensitive way of detecting foreign bodies and occasionally linear foreign bodies can be diagnosed using this non-invasive modality (Fig. 29-4). Ultrasonography may also be used to evaluate gastrointestinal motility, the presence of fluid distension, and diagnosing foreign bodies with characteristic acoustic signals.5 Ultrasonography has been identified as a highly sensitive indicator of intussusception. On lateral views the intussusceptum is easily identified and on axial views a characteristic ‘bull’s eye’ image is seen (Fig. 29-5). However, ultrasonography may not always accurately predict the presence of intestinal perforation.6 Figure 29-2 Lateral abdominal radiograph of a kitten with an intussusception. Black arrows indicate the ratio of the maximum diameter loop of small intestine (30 mm) divided by the dorsoventral height of the cranial endplate of L2 (9 mm) to be >3.0, making this suggestive of complete intestinal obstruction.4 Figure 29-3 Contrast study of a cat with small intestinal pleating secondary to ingestion of linear foreign body. (Courtesy of Stephen Birchard, The Ohio State University.) Figure 29-4 Ultrasound image of a linear foreign body (arrow) in a 10-month-old female cat. (Courtesy of the University of Cambridge.) Approximately half of the gastrointestinal foreign bodies in cats are caused by non-linear foreign bodies.6 Non-linear foreign bodies commonly identified in the cat include coins, ear-plugs, small toys, almonds, or fishing tackle. Small intestinal obstruction by a foreign body can be complete or partial and the clinical signs vary in severity as a result of the level and degree of obstrucsion. The degree of obstruction also defines the variability in the presenting clinical signs. Abdominal palpation may identify intestinal distension, a palpable object, or abdominal pain. Cats commonly swallow coins but these usually do not exit the stomach. Rubber balls, cellophane, or chew toys tend to pass slowly or not at all and are more likely to cause complete mechanical obstruction requiring enterotomy or enterectomy. Opaque objects are easily identifiable on plain radiographs but many foreign bodies are radiolucent. Less dense foreign bodies are sometimes missed on ultrasound. If contrast radiography is needed for diagnosis aqueous iodine contrast should be used. Most proximal small intestinal obstructions are visible within six hours whereas a 24 hour study may be indicated for more distal obstructions. Surgical management of gastrointestinal foreign bodies varies depending on the type and location of the foreign body. Sharp foreign bodies such as straight pins, safety pins, bones, or glass will often pass through the gastrointestinal tract without creating intestinal perforation unless they are attached to thread or yarn. Linear foreign bodies, caused by such items as fishing line, meat wrappers, or sewing yarn, present a difficult surgical problem. Some linear foreign bodies will pass spontaneously but the trailing end often catches over the base of the tongue or in the stomach and acts as an anchor.7 Intestinal peristalsis moves the foreign body aborally resulting in bowel plication. Linear foreign bodies should be managed by initially identifying and releasing the anchor point, either from the tongue, or via a gastrotomy to free the wadded string or fishing line from its gastropyloric anchor (see Chapter 28). Multiple enterotomies are sometimes required to facilitate complete removal of the foreign body. If too few enterotomies are made, with too much traction placed on the string, the mesenteric border may be perforated in an area which is difficult to explore and suture. Occasionally the string has already cut through at several locations and peritonitis is evident. In 64 cases of linear foreign bodies in cats, most animals were less than four years old. Surgery and multiple enterotomies or enterectomy were used in 90% of the cases and 84% of the cases survived. However, the survival rate in cats that had concurrent bowel perforations was only 50%.2 A single catheter technique for removal of linear foreign bodies can often be used successfully in cats, but survival rates for this technique are not known.8 There have been failures associated with the single catheter technique for removal of linear foreign bodies. In one case report, passage of the catheter created tearing of the mesenteric border at the location where the linear foreign body was embedded, thus necessitating resection and anastomosis of 60% of the small intestine.9 Likewise, in long-standing cases of intestinal linear foreign body, fibrosis may occur so that even after its removal the bowel retains its pleated configuration. In these cases, massive intestinal resection and anastomosis may be necessary. The exact pathogenesis of the condition is unknown but theories include a local incongruency of the intestine caused by induration (secondary to neoplasia), or spasticity (intestinal parasitism), or anatomical diameter change occurs in which a proximal bowel segment invaginates (intussusceptum) into a distal section of bowel (intussuscipiens) (Fig. 29-6). Intussusceptions are also seen with increasing frequency after laparotomy on elective or non-elective intra-abdominal procedures. Clinical signs depend on the completeness and level of obstruction. In older cats intussusception is often associated with intestinal neoplasia (Fig. 29-7). The intussusception often becomes irreducible as a result of the congestion and outpouring of fibrinous exudate from the serosa. Although the invaginated bowel may become devitalized, perforation is rare because the outer ensheathing layer retains its viability and the adhesions seal the proximal border of the intussusception. Occasionally spontaneous recovery occurs when the non-viable intussusceptum is sloughed and patency of the lumen is recovered. Figure 29-6 Illustration of typical anatomic configuration of a single intussusception with the inner invaginated intussusceptum and outer ensheathing intussuscipiens. (Samantha J Elmhurst BA Hons/www.livingart.org.uk from Stanley BR. The small intestine. In Williams JM and Niles JD. BSAVA Manual of Canine and Feline Abdominal Surgery. Gloucester 2005; p 107.) Figure 29-7 Intraoperative image of a mid-jejunal intussusception in a 13-year-old British short-haired cat. The outcome of 20 cats with gastrointestinal tract intussusception identified that this disease differs significantly from intussusception in dogs.10 Intussusception in cats appears to be a biphasic disease, with one group of cats being less than one year of age and having concurrent intestinal endoparasitism. The second group was over six years of age and the majority of the older cats had either intestinal lymphoma or inflammatory bowel disease as the common etiology for their intussusception. Clinical signs included anorexia, lethargy, vomiting, dehydration, poor body condition, and signs of abdominal pain. Diagnosis was made using a combination of abdominal palpation, abdominal radiography, and abdominal ultrasonography. Most specific was abdominal ultrasonography, which was diagnostic in seven of seven cases in which it was performed. Jejunojejunal was the most common site of intussusception and no intussusceptions were found proximal to the duodenum. Thirteen cats were taken to surgery and 11 of these cats required intestinal resection and anastomosis. The need for prophylactic bowel plication or enteropexy remains controversial. Bowel plication involves laying the bowel side by side in a series of gentle loops. The loops are sutured together on their antimesenteric border using simple interrupted sutures of non-absorbable 4/0 suture material that penetrate the seromuscular layers of bowel but do not enter the lumen.11 However, a retrospective report in dogs indicated that intestinal plication might not be necessary since the risk of complications is higher after plication and there was only a slight reduction in the recurrence rate of intussusception.12 Pathologic twisting of bowel on its mesenteric axis is termed intestinal or mesenteric volvulus. Mesenteric volvulus is rare in cats. There have been five cases reported in the literature with two survivors. Reported clinical signs included acute onset of abdominal distension in the presence of shock, anemia, air-filled loops of bowel, and vomiting or retching. Of the three non-survivors, two cases were diagnosed at necropsy and the third cat failed to survive surgery. Of the two successful surgical cases one was a 16-month-old domestic short hair and the other a five-year-old Bengal. Both animals had acute abdominal signs and presented in a very anemic state with packed cell volumes below 10%. Both animals received blood transfusions and had resection of the proximal jejunum and the ileum. The lengths of resected intestines were 35 and 40 cm, respectively. Postoperatively, both cats had chronic diarrhea for a period of time, which ultimately improved but did not completely resolve. Based on these two cases it appears that cats can survive mesenteric volvulus so long as surgery is performed promptly after appropriate stabilization of the cat, including blood transfusion (see Chapter 5) and some of the small intestine including the duodenum and upper jejunum is retained.13 Adenomatous polyps of the duodenum have been reported in cats. They were older cats with a median age of about 12 years and the Siamese and Himalayan breeds were over represented. The polypoid mucosal masses were located in the upper duodenum and tended to cause vomiting and weight loss. When the lesions ulcerate hematemesis may occur. About half the cats became anemic secondary to chronic blood loss. Diagnosis was made on contrast radiography or endoscopically. This is a surgical disease and requires excision of the lesions through an enterotomy incision or via resection and anastomosis. The lesions are benign but regrowth is possible if inadequate submucosal resection occurs. In one case study, 13 of 18 cats were cured, four had recurring signs and one cat died following surgery.14 The author has also seen benign adenomatous polyps located in the jejunum which caused a secondary intussusception (Fig. 29-8). A large case series of 26 cats with FIP had concurrent solitary mural intestinal lesions that mimicked intestinal neoplasia.15 The majority of these cats had the lesions removed during exploratory laparotomy although some of the lesions were diagnosed at necropsy. The presumptive diagnosis in most of the cats was a solitary intestinal lesion most consistent with neoplasia. However, results of histologic examination revealed that the lesions were predominantly granulomatous, nodular, firm and white, and extended throughout the wall of the intestine on histologic examination (Fig. 29-9). Associated lymph nodes were enlarged and had evidence of inflammation. Serology was positive for the FIP virus in all 26 cats. The clinical outcome of these cats was poor. Many cats were euthanized at the time of surgery and all cats that were recovered from anesthesia died within nine months of the surgical procedure. Many of the cats also had signs of multi-systemic FIP. The clinical implications of this study are the focal nature of intestinal lesions with this type of FIP is easily confused with neoplasia at the time of surgery and long-term prognosis is poor.
Small intestines
Surgical anatomy
General considerations
Clinical findings
Diagnostic imaging

Surgical diseases of the small intestines
Foreign bodies
Non-linear foreign bodies
Linear foreign body
Intussusception

Mesenteric volvulus
Non-neoplastic lesions
Adenomatous polyps
Feline infectious peritonitis (FIP) granulomas
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Small intestines




