chapter 14 Small Animal Pelvis and Hind Limb
Lateral View
The patient is placed in lateral recumbency with the side of interest closest to the cassette (Figs. 14-1 and 14-2). A foam wedge should be placed between the patient’s stifle joints to keep the femurs parallel with the cassette. A foam wedge also alleviates rotation and ensures that the two sides of the pelvis are superimposed. To distinguish the right femur from the left on the finished radiograph, the limb closest to the cassette should be pulled slightly cranial and the top leg slightly caudal. This staggering of the femurs is especially important if the patient has a hip luxation and one femur needs to be differentiated from the other. The field of view should include the entire pelvis and a portion of the lumbar spine and the femurs. The pelvis should be centered in the middle of the cassette.

BEAM CENTER: Over greater femoral trochanter
Ventrodorsal View
Frog-leg projection.
The patient is placed in dorsal recumbency (Figs. 14-3 and 14-4). A V trough is a useful positioning device to maintain bilateral symmetry. The pelvic limbs can assume a normal, flexed position. The femurs should be at a 45-degree angle to the spine and can be secured in that position by placing sandbags over the tarsal joints. Positioning the limbs identically is important to maintain symmetry.

Extended projection.
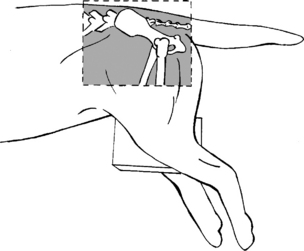
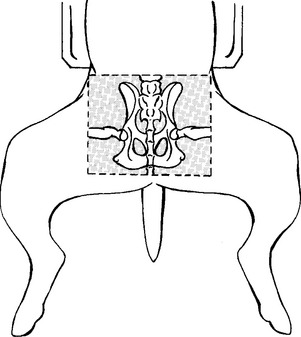
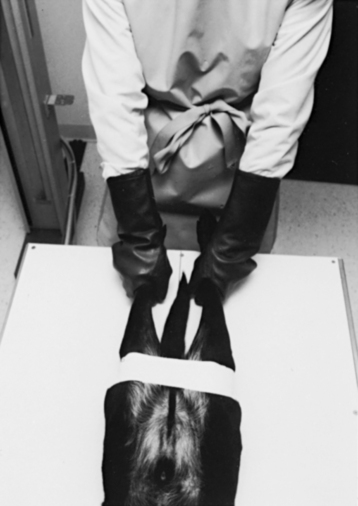
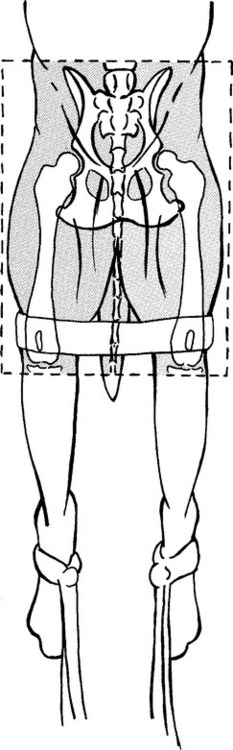
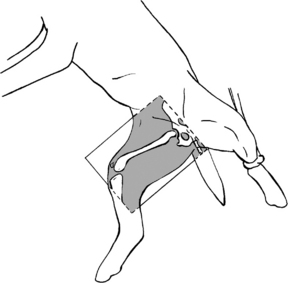
A number of steps are necessary to achieve proper pelvis positioning. The patient is placed in dorsal recumbency with its back in a V trough or maintained with the aid of sandbags. The pelvic limbs are flexed into a frog-leg position, and the tarsal joints are grasped firmly. At this point the stifle joints are rotated medially toward each other. When the stifles are within 1 or 2 inches of each other, the limbs are extended caudally until the femurs are parallel with the cassette or until resistance is encountered. The hind legs can be secured with adhesive tape or handheld with the use of lead gloves (Figs. 14-5 through 14-8).

Figure 14-5 Ventrodorsal extended view of the pelvis: Place the patient in the ventrodorsal frog-leg position.


For correct positioning (Figs. 14-9 and 14-10), the following criteria must be met:

BEAM CENTER: Over level of pubis and acetabulum
MEASUREMENT: Over acetabulum (groin)
BEAM CENTER: Caudal portion of ischium
The PennHIP method.
In the early 1980s Dr. Gail Smith and a team of researchers at the University of Pennsylvania School of Veterinary Medicine began a scientific investigation to determine a more reliable phenotype to predict canine hip dysplasia. PennHIP, the result of that research effort, refers to a specific diagnostic technique, as well as a provider network and database of hip laxity information. The PennHIP method has been shown to provide a more repeatable and reliable indication of a dog’s passive hip laxity than is possible with the hip extended radiograph. The stress radiographic procedure consists of three views: the standard extended view (Fig. 14-11), a compressionview with a neutral position, and a distraction view in the same neutral hip position (Figs. 14-12 and 14-13). In the absence of existing degenerative disease, laxity is the single most important component in predicting a dog’s susceptibility to canine hip dysplasia.

Figure 14-11 Traditional hip extended view. Orthopedic Foundation for Animals (OFA) rating of “good.”
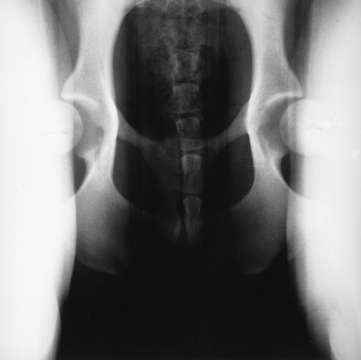
Figure 14-12 PennHIP distraction view of the same dog. Note the marked laxity present on this view that was not evident from the extended hip view in Figure 14-11.

Lateral View
The patient is placed in lateral recumbency with the affected limb closest to the cassette. The opposite limb is abducted and rotated out of the line of the x-ray beam (Figs. 14-14 and 14-15). A foam pad placed under the proximal tibia can alleviate any rotation of the femur. The field of view should include the hip joint, femur, and stifle joint.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


